
Foods to help balance fatty liver
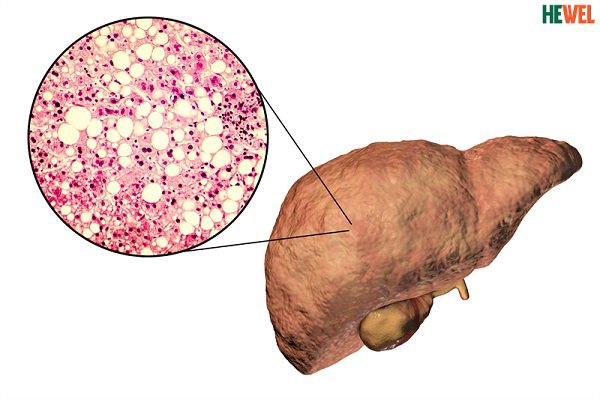
1. What is fatty liver disease?
Fatty liver is a common disease with an increasing incidence. Fatty liver disease, if not detected and treated early, can lead to hepatitis, cirrhosis, and even liver cancer. Therefore, it is best to prevent disease with foods that help balance fatty liver.
2. Fatty liver eat what?

3. Lifestyle changes in fatty liver disease
Control and maintain ideal weight: Regular monitoring of weight as well as weight gain is essential in controlling fatty liver disease, helping to control fatty liver disease. Regulates excess fat accumulation in the liver. When you are overweight or obese, you need to actively lose weight to achieve your ideal weight.
The BEST Drink for a Fatty Liver
Dandelion root tea is also believed by some to help detoxify the liver and relieve symptoms of liver disease. To make dandelion tea, you can steep one tablespoon of dandelion roots or flowers in five ounces of boiling water for 30 minutes, then strain or drink the mixture.
Easy Liver Cleanse Recipe: Detox Naturally with Lemon and Olive Oil
You only need to look at simple liver cleanse recipes that combine the flavorful combination of lemon and olive oil. This cleansing method supports liver function and promotes general well-being by utilizing the natural detoxifying qualities of these herbs in a gentle yet effective way.
Olive oil and lemon are the main ingredients in the main cuisine of European restaurants. Many people say that the combination of lemon juice and olive oil can treat many diseases like gallbladder stones.
Furthermore, research has looked at the possible health benefits of the components in lemon juice and olive oil independently.
This article will talk about the fact that studies support the purported health benefits of combining lemon juice with olive oil.
We’ll also review the olive oil lemon juice liver cleanse recipe.
Discover the Mutual Impact of Olive Oil and Lemon on liver
There we will learn about the combination of lemon juice and olive oil. Lemon and olive oil make an extremely unique combination. It is open to all, committed, and productive for the skin, liver, and even blood flow.
Let’s first explore the two fruits independently: The ability of lemon to act as an acidifying agent is its power.
The human body can become acidified if its pH level is out of balance, which can have major negative effects on health. Hyperacidity is countered and the pH value is adjusted during alkalizing. Therefore, sick cells typically lose their strength as well as their breeding ground.
There are many liver cleansing recipes with lemon juice and olive oil. Because these are the most easily used liver detox. Lemon Liver detox works properly to clean liver stones and many other harmful small agents.
Olive oil and Lemon Juice Liver Cleanse Recipe
Ingredients:
- 1/2 cup of extra virgin olive oil
- 1/4 cup of freshly squeezed lemon juice
- 1-2 cloves of minced garlic
Instructions:
- Before beginning the cleanse, fast for a minimum of 12 hours to enable your liver to get ready for detoxification.
- In a bowl, thoroughly mix the olive oil, lemon juice, and minced garlic.
- During one to two hours, take one tiny serving (about one to two tablespoons) of the olive oil mixture every fifteen minutes.
- After you’ve finished the olive oil mixture, lie on your right side with your knees pulled up to your chest for half an hour.
- Spend the rest of the evening sleeping so that the cleanse has time to work.
How do you know that this combination is best for you?
Some research shows that eating lemon juice and olive oil together has health benefits. Many claim that they can aid in weight loss, treat and prevent gallstones, and perform cleanses and detoxes.
Let’s look at each of these claims properly.
Cleansing and Detoxification Ideas
A fast internet search will bring up a variety of recipes claiming to use lemon juice, olive oil, or both to detox and cleanse. It is said that waste and toxins that have accumulated in your body over time are taken out by cleanses and detoxes.
On the other hand, research on the potential cleansing and detoxifying effects of lemon juice and olive oil does not seem to be very extensive.
When compared to those who consumed other plant oils, the researchers discovered that those who consumed olive oil during the study period had greater levels of HDL (good) cholesterol and lower levels of LDL (bad) cholesterol in their blood.
In this article, we will give you the natural liver detox recipe for your best hygiene.
However, the polyphenols and antioxidants in lemon juice and olive oil could be referred to as “cleansing” because they “clean up” or neutralize dangerous free radicals. Which otherwise damages cells and may be a factor in sickness and disease.
Lemon and olive oil are recommended as the best quick liver detox. The human body uses a variety of biological processes to get rid of pollutants and keep itself operating at its best.
I suggest eating a diet that is rich in fruits, vegetables, whole grains, legumes, nuts, seeds, and lean protein sources to support your body’s optimal functioning.
Weight Loss
Vitamin C is rich in lemon juice. 38.7 mg, or 43% of the Recommended Dietary Allowance (RDA) for men and 52% of the RDA for women, is present in a 3-ounce (100-gram) serving. Vitamin C plays a crucial role in the body’s synthesis of carnitine.
A substance called carnitine is responsible for moving fat molecules into cells so they may be broken down and used as an energy source. Thus, a low vitamin C consumption could result in less fat being broken down. For
weight loss, many quick liver detox drinks are also available in the market.
Health Benefits of using Liver oil and Lemon Cleanse
What health advantages are associated with gallbladder cleansing?
To prevent gallstones, certain supporters of alternative healthcare advise liver cleansing. They maintain that the liver releases the gallstones as a result of the liver cleaning.
The gallstones should then ideally pass via the stool. This would mean that the patient would have fewer gallstones left to produce uncomfortable symptoms and might be able to avoid surgery.
There are various kinds of liver cleanses. Alternative medicine practitioners provide many ” liver detox recipes” and traditional treatments online.
- Olive oil and lemon juice. Using this method, you will fast for 12 hours during the day and then drink 4 tablespoons of olive oil and 1 tablespoon of lemon juice, eight times every 15 minutes, starting at 7 p.m.
- Vegetables and apple juice. Using this method, all you consume till five o’clock in the evening is apple and vegetable juice. Every fifteen minutes after 5 p.m., ingest eight ounces of olive oil by consuming 18 milliliters (ml) of olive oil mixed with 9 ml of lemon juice.
In these points, we tell you about the easy liver detox remedy that you can use at home easily.
How might a liver cleanse cause side effects?
Depending on the “recipe” one follows, cleansing may have different adverse effects. For example, a lot of individuals cleanse their livers using olive oil. When consumed in excess, this may have a laxative effect.
The following symptoms are possible for some people to experience after a gallbladder cleanse:
- Diarrhea vomiting nausea
- Depending on the herbs or other things someone utilizes in their cleanse, there could be additional negative consequences.
Furthermore, a person may perform a gallbladder cleansing yet still not be able to get rid of their gallstones. To prevent their symptoms from getting worse or an infection in their gallbladder. They probably need to have surgery at that point.
How to liver cleanse at home?
To support your liver’s natural detoxification activities and enhance general well-being. Liver cleansing at home might be a quick and easy solution. A possible strategy is to consume fewer processed meals, alcoholic beverages, and added sugars while increasing your intake of foods high in fiber, such as fruits, vegetables, and whole grains.
Furthermore, drinking lots of water throughout the day to stay hydrated promotes liver function and the removal of toxins. Herbal teas that you can drink regularly, like milk thistle or dandelion root, are also well-known for their liver-cleansing qualities. Different liver detox tea recipes are also present on the internet.
How much olive oil for detox?
Depending on things like tolerance levels, individual health status, and particular detox procedures, there are differences in the suggested quantity of olive oil for detoxification. In general, it’s important to balance safety and efficacy while using olive oil in a detox program.
As part of a detox treatment, it is generally recommended to ingest 1-2 tablespoons of extra virgin olive oil daily.
The body’s natural detoxification processes are supported by this moderate amount of beneficial substances, which do not overburden the system. These components include antioxidants and monounsaturated fats.
Conclusion
Cleanse Your Liver
In addition to lifestyle changes, nutrition can have an impact on liver health. Check out these beverages that can aid in improving liver function.
Your liver plays many important roles in your physical health. It aids in digestion and metabolism and acts as a filter for the blood, breaking down harmful substances into waste that is expelled from the body through urine and stool.
According to the Mayo Clinic, symptoms of liver dysfunction include:
- Skin and eyes that appear yellowish (jaundice)
- Abdominal pain and swelling
- Swelling in the legs and ankles
- Itchy skin
- Dark urine color
- Pale stool color
- Chronic fatigue
- Nausea or vomiting
- Loss of appetite
- Tendency to bruise easily
Liver disease can be genetic. Other factors like viral infections, age, obesity, or excessive alcohol use may also cause liver damage or dysfunction. If left untreated, this damage can be fatal.
The good news is the liver is the only organ in the body with the ability to regenerate new cells and repair damaged ones. Repairing liver damage can be challenging; however, it is possible through consistent diet and lifestyle changes. These include:
- Maintaining a healthy weight
- Eating nutritious food and having a balanced diet
- Getting regular exercise
- Avoiding harmful additives and chemicals
- Avoiding excessive or continued alcohol or illegal drug use (damage from alcohol abuse can cause irreversible cirrhosis of the liver)
Also, many beverages, such as water, tea, and grapefruit juice, can be beneficial for your overall health and may aid detoxification of the body and liver.
Water
Staying properly hydrated is an important factor in maintaining a healthy liver. Dehydration can greatly affect liver function, especially the ability to detoxify blood. On average, you should drink eight to ten glasses of water a day; those with health conditions may need to increase their water intake beyond the recommended amount.
Teas
There are a few natural teas that may assist in liver function. Several popular and possibly beneficial teas for liver health include:
- Lemon Ginger Tea – reduces the risk of liver disease
- Peppermint Tea – improves digestion and detoxifying functions of the liver
- Green Tea – reduces the accumulation of lipids in the liver and contains antioxidants
Research the health effects and benefits of specific teas or discuss recommendations with your health care provider to ensure safe recommended use.
Grapefruit Juice
Grapefruit juice contains specific antioxidants that stimulate the liver and help filter and excrete chemicals from the body. Grapefruit also contains flavonoids naringin and naringenin, which have anti-inflammatory and antioxidant properties that may help protect the liver. However, it is recommended to not consume more than six ounces of grapefruit juice per day. Grapefruit juice also interacts with many prescription medications, so please check with your doctor or pharmacist and read your medication warning labels before adding it to your diet.
Turmeric Water
Turmeric is a commonly used supplement that may decrease inflammation and assist with liver repair, due to its ability to help flush out harmful toxins while decreasing fat buildup in the liver. For safe use, medical studies recommend mixing one to three grams of dried turmeric root in hot water each day for up to three months.
Lemon Water
Many citrus fruits, including lemon, can be added to water to help stimulate and flush out the liver. Lemons are high in nutrients like vitamin C and antioxidants. To help prevent liver disease, enjoy four to six tablespoons of lemon juice mixed with water each day.
Ginger Water
Ginger helps protect your liver and reduces inflammation in the body. It may also boost immunity and improve digestive health. The recommended consumption is less than four grams of ginger per day, mixed with warm or cold water.
As with any change in nutritional intake or supplement use, please use caution. Some people may experience unwanted results or side effects, and some herbs and foods may interact with certain medications. Also, the information presented above is based on adult studies and should not be used for children. Research any supplements and consult a health care professional before making abrupt changes to your diet or lifestyle. source
DRINK 1 CUP PER DAY to Remove Fat from Your Liver – Dr. Berg
Many people have a fatty liver and don’t even know it.
Today I want to help you better understand the liver and how to remove fat from the liver. The purpose of the liver is to break down toxins into harmless particles. A fatty liver can become heavy and enlarged. This can lead to fullness under the right rib cage and shoulder pain.
Important functions of the liver:
- It makes bile
- It helps convert thyroid hormones
- It buffers excess sex hormones
Bile is made by the liver, and it helps you break down fat. A lack of bile can lead to a lot of various health problems. Bile is also very important to keep fat out of the liver. Anything you can do to help increase bile reserves will help you remove liver fat. You may even want to take purified bile salts. Keep in mind that the ketogenic diet and intermittent fasting can help remove fat from the liver. I believe this is essential if you have a fatty liver.
A great shake to keep fat off the liver: Ingredients (organic if possible):
- 2 cups kale (frozen)
- 1 cup blueberries (frozen)
- 1 cup water
- 1 cup plain whole-milk kefir (organic and grass-fed if possible)
Instructions: Blend all of the ingredients in a blender for a couple of minutes. Drink once a day in combination with a Healthy Keto diet and intermittent fasting.
Protective Effects of Lemon Juice on Alcohol-Induced Liver Injury in Mice
Abstract
Chronic excessive alcohol consumption (more than 40-80 g/day for males and more than 20-40 g/day for females) could induce serious liver injury. In this study, effects of lemon juice on chronic alcohol-induced liver injury in mice were evaluated. The serum biochemical profiles and hepatic lipid peroxidation levels, triacylglycerol (TG) contents, antioxidant enzyme activities, and histopathological changes were examined for evaluating the hepatoprotective effects of lemon juice in mice. In addition, the in vitro antioxidant capacities of lemon juice were determined. The results showed that lemon juice significantly inhibited alcohol-induced increase of alanine transaminase (ALT), aspartate transaminase (AST), hepatic TG, and lipid peroxidation levels in a dose-dependent manner. Histopathological changes induced by alcohol were also remarkably improved by lemon juice treatment. These findings suggest that lemon juice has protective effects on alcohol-induced liver injury in mice. The protective effects might be related to the antioxidant capacity of lemon juice because lemon juice showed in vitro antioxidant capacity.
1. Introduction
Alcohol abuse and alcoholism could lead to serious health and socioeconomic problems worldwide. Chronic excessive alcohol consumption (more than 40–80 g/day for males and more than 20–40 g/day for females) could lead to several illnesses, such as gastrointestinal damage, pancreatitis, alcoholic liver disease, neurologic disorders, diabetes mellitus, and cancer [1, 2]. Among these diseases, alcoholic liver disease has attracted more attention due to its high morbidity and mortality. Alcoholic liver disease is a major type of chronic liver disease throughout the world and can progress to liver cirrhosis and liver cancer.
Chronic alcohol consumption can generate abundant reactive oxygen species (ROS), including superoxide anion radical (O2−•), hydroxyl radical (OH•), and hydrogen peroxide (H2O2). The ROS can react with most cellular macromolecules and subsequently cause cellular damage [3]. Therefore, the excessive ROS induced by alcohol is regarded as an important factor in the development of alcohol-induced liver injury. Various enzymatic and nonenzymatic antioxidants are related to protecting cells against ROS. Antioxidant enzymes include catalase (CAT), superoxide dismutase (SOD), and glutathione peroxidase (GPx), and nonenzymatic antioxidants include glutathione (GSH), vitamin E, ascorbate, vitamin A, and ubiquinone [4]. Nonenzymatic antioxidants can be enhanced by antioxidant intake. In recent years, many natural products that have abundant antioxidants were reported to possess the effect of scavenging free radicals and protecting the liver from oxidative damage [4, 5].
Lemon is a popular fruit consumed as juice and contains high contents of vitamins and polyphenols (mainly flavonoids), such as hesperidin, eriocitrin, naringin, neohesperidin, rutin quercetin, chlorogenic acid, luteolin, and kaempferol [6]. The in vivo and in vitro experiments have shown that lemon has various health benefits, such as anticancer effect, antimicrobial effect, lipid-lowering effect, and protective effect against cardiovascular diseases [6]. In addition, lemon is used to treat liver ailments in tribal medicine [7]. However, effects of lemon juice on chronic alcohol-induced liver injury have not been reported in the literature. The objective of this study is to investigate the effects of lemon juice on chronic alcohol-induced liver injury in mice. In addition, the in vitro antioxidant capacities of lemon juice were evaluated. The results of this study could supply valuable information for the general public to reduce harm of alcohol consumption.
2. Materials and Methods
2.1. Chemicals and Reagents
The compounds 6-hydroxy-2,5,7,8-tetramethylchromane-2-carboxylic acid (Trolox), 2,2′-azinobis(3-ethylbenzothiazoline-6-sulfonic acid) diammonium salt (ABTS), 2,4,6-tri(2-pyridyl)- S-triazine (TPTZ), quercetin, gallic acid, and Folin–Ciocalteu’s phenol reagent were purchased from Sigma-Aldrich (St. Louis, MO, USA). Assay kits for the determination of SOD, lipid peroxidation, CAT, and TG contents were purchased from Nanjing Jiancheng Bioengineering Institute (Nanjing, China). Other chemicals were of analytical grade.
2.2. Materials
Lemon was obtained from markets in Guangzhou, China. The fruit was cleaned with deionized water. The edible portion was weighed precisely and mixed with deionized water (1 : 1, m/v), and the mixture was ground into a homogenate with a homogenizer. Then, the homogenate was centrifuged at 5,000g for 10 min, and the supernatant was obtained. The supernatant was used for the measurement of antioxidant capacity, total phenolic contents (TPC), and total flavonoid contents (TFC) and for animal experiments. Moreover, in animal experiments, the original supernatant and the diluted supernatant (1 : 5 and 1 : 10, m/v) were used as the high, medium, and low dose, respectively. The lemon juice was freshly prepared before gavage every time.
2.3. Animal Study
Male C57BL/6 mice (20–25 g) were employed in this study. Thirty mice were randomly divided into 5 groups, each group containing 6 mice. They were maintained in a SPF laboratory animal room, which kept a 12 h light/dark cycle at 22 ± 0.5°C with 40%–60% relative humidity. The animal study was performed according to the “Principles of Laboratory Animal Care” and approved by the Institutional Animal Ethics Committee of Sun Yat-sen University. The model group was treated daily with ethanol and distilled water (10 mL/kg) at the same time; the lemon juice treatment groups were treated daily with different concentrations (high dose 1 : 1 (m/v), medium dose 1 : 5, and low dose 1 : 10) of lemon juice (10 mL/kg) and ethanol simultaneously; the control group was treated daily with isometric distilled water. The model group and the lemon juice treatment groups were given ethanol according to the following ways: 35% ethanol (v/v) at a dose of 3 g/kg body weight for 7 days, 40% ethanol (v/v) at a dose of 4 g/kg body weight for the next 7 days, and 52% ethanol (v/v) at a dose of 5 g/kg body weight on the 15th day [8]. All the intervention methods were intragastric administration. The blood and liver were collected from mice 9 h after the last ethanol administration. The blood sample was centrifuged at 4,000g for 10 min and the serum was collected. The obtained serums were stored at −22°C before determination. A piece of tissue was taken from liver and fixed in 4% paraformaldehyde, and then the remaining liver tissue was stored at −22°C until use.
2.4. Measurement of Biochemical Parameters in the Serum
The levels of ALT, AST, and TG in serum were determined by a Hitachi-7180 automated biochemistry analyzer (Hitachi, Japan) with the corresponding reagent kit.
2.5. Measurement of TG and Antioxidant Enzyme Activities in the Liver
The levels of TG, SOD, and CAT in liver tissue were measured using the commercial detection kits according to the manufacturer’s instructions.
2.6. Measurement of Lipid Peroxidation Levels in the Liver
The levels of lipid peroxidation in liver tissue were measured by thiobarbituric acid (TBA) method using the commercial detection kits according to the manufacturer’s instructions. The reference standard was malondialdehyde (MDA), and the results were expressed as nmol MDA equivalent/mg prot.
2.7. Liver Histopathological Assessment
The liver tissue fixed in 4% paraformaldehyde was embedded in paraffin, sectioned into 5 μm thickness, and stained with hematoxylin-eosin (H&E) for evaluation of histopathological changes. The histopathological changes of stained liver slices were observed under a bright-field microscope.
2.8. Ferric-Reducing Antioxidant Power (FRAP) Assay
The FRAP assay was performed based on the method described in the literature [9]. In brief, the FRAP reagent was prepared from 10 mmol/L TPTZ solution, 20 mmol/L iron(III) chloride solution, and 300 mmol/L sodium acetate buffer solution (pH 3.6) in a volume ratio of 1 : 1 : 10, respectively. 100 μL of the diluted sample was added to 3 mL of the FRAP reagent and the mixture was measured after 4 min at 593 nm. The standard curve was established using FeSO4 solution, and the results were expressed as μmol Fe(II)/g dry weight of lemon.
2.9. Trolox Equivalent Antioxidant Capacity (TEAC) Assay
The TEAC assay was carried out according to the procedure in the literature [10]. Briefly, the ABTS•+ stock solution was prepared from 2.45 mmol/L potassium persulfate and 7 mmol/L ABTS solution in a volume ratio of 1 : 1 and then placed in the dark for 16 h at room temperature. The ABTS•+ working solution was prepared by diluting the stock solution, and the absorbance of ABTS•+ working solution was 0.710 ± 0.05 at 734 nm. 100 μL of the diluted sample was mixed with 3.8 mL ABTS•+ working solution, and the absorbance of the mixture was measured at 734 nm after 6 min, and the percent of inhibition of absorbance at 734 nm was calculated. The reference standard was Trolox, and the results were expressed as μmol Trolox/g dry weight of lemon.
2.10. Determination of TPC
TPC were measured according to the literature [11]. Briefly, 0.50 mL of the diluted sample was added to 2.5 mL of 0.2 mmol/L Folin–Ciocalteu reagent. After 4 min, 2 mL of saturated sodium carbonate solution was added. After incubation for 2 h at room temperature, the absorbance of the mixture was measured at 760 nm. The reference standard was gallic acid, and the results were expressed as mg gallic acid equivalent (GAE)/g dry weight of lemon.
2.11. Determination of TFC
TFC were measured according to the literature [12]. In brief, 0.50 mL of the sample was mixed with 1.5 mL of 95% ethanol (v/v), 0.1 mL of 10% aluminum chloride (w/v), 0.1 mL of 1 mol/L potassium acetate, and 2.8 mL of water. After incubation for 30 min at room temperature, the absorbance of the mixture was determined at 415 nm. The reference standard was quercetin, and the results were expressed as mg of quercetin equivalent (QE)/g dry weight of lemon.
2.12. Statistical Analysis
Statistical analysis was carried out by one-way analysis of variance (ANOVA) with post hoc LSD test using SPSS 13.0 software. p < 0.05 was regarded as significant.
3. Results
3.1. Effects of Lemon Juice on the Levels of ALT and AST in Serum
As shown in Figure 1, the administration of alcohol led to a significant (p < 0.05) elevation of alanine transaminase (ALT) and aspartate transaminase (AST) levels in serum of the model group compared with that of the control group. The administration of low and medium concentration of lemon juice slightly prevented the elevation of serum level of AST, while a high dose of lemon juice significantly (p < 0.05) decreased it. At the same time, the prevention of the elevation of serum levels of ALT was observed significantly (p < 0.05) in medium and high concentration of lemon juice group and displayed a dose-effect relationship.

Effects of lemon juice on the levels of AST (a) and ALT (b) in serum of mice. Control: normal group; Model: alcohol group; LL: alcohol and low dose of lemon juice group; LM: alcohol and medium dose of lemon juice group; LH: alcohol and high dose of lemon juice group. ∗ means the levels of parameters in the model group were significantly (p < 0.05) different from those of the control group. # means the levels of parameters in the treatment group were significantly (p < 0.05) different from those of the model group.
3.2. Effects of Lemon Juice on the Levels of TG in Serum and Liver
Triacylglycerol (TG) content in serum was significantly (p < 0.05) increased in the model group compared with that in the control group (Figure 2(a)). Administration of lemon juice reduced the accumulation of TG in a dose-dependent manner, especially in high concentration of lemon juice group (p < 0.05). In addition, hepatic TG content was significantly (p < 0.05) increased in model group compared with that in the control group (Figure 2(b)). Administration of medium and high concentration of lemon juice significantly (p < 0.05) reduced the accumulation of hepatic TG in a dose-dependent manner.

Effects of lemon juice on TG contents in serum (a) and liver (b). Control: normal group; Model: alcohol group; LL: alcohol and low dose of lemon juice group; LM: alcohol and medium dose of lemon juice group; LH: alcohol and high dose of lemon juice group. ∗ means the levels of parameters in the model group were significantly (p < 0.05) different from those of the control group. # means the levels of the parameters in the treatment group were significantly (p < 0.05) different from those of the model group.
3.3. Effects of Lemon Juice on Liver Lipid Peroxidation Levels
The lipid peroxidation levels in liver tissue are shown in Figure 3. Compared with that of the control group, there was a significant (p < 0.05) increase in the lipid peroxidation level of the model group. The administration of lemon juice significantly (p < 0.05) decreased the level of lipid peroxidation in a dose-dependent manner.

Effects of lemon juice on hepatic lipid peroxidation level in mice. Control: normal group; Model: alcohol group; LL: alcohol and low dose of lemon juice group; LM: alcohol and medium dose of lemon juice group; LH: alcohol and high dose of lemon juice group. ∗ means the levels of the parameters in the model group were significantly (p < 0.05) different from those of the control group. # means the levels of the parameters in the treatment group were significantly (p < 0.05) different from those of the model group.
3.4. Effects of Lemon Juice on Liver Antioxidant Enzyme Activities
Figure 4 represents the results of hepatic antioxidant enzyme activities in five groups. The SOD level in the liver increased significantly (p < 0.05) in the model group compared with that in the control group. The CAT level in the liver decreased only slightly (p > 0.05) in the model group compared with the control group in this study. However, treatment with lemon juice significantly (p < 0.05) decreased the levels of SOD and CAT compared with those of the model group. In addition, all the biochemical parameters are summarized in Table 1.

Effects of lemon juice on the activities of SOD (a) and CAT (b) in liver. Control: normal group; Model: alcohol group; LL: alcohol and low dose of lemon juice group; LM: alcohol and medium dose of lemon juice group; LH: alcohol and high dose of lemon juice group. ∗ means the levels of the parameters in the model group were significantly (p < 0.05) different from those of the control group. # means the levels of the parameters in the treatment group were significantly (p < 0.05) different from those of the model group.
Table 1
Effects of lemon juice on the levels of several biochemical parameters.
| Parameters | Control | Model | LL | LM | LH |
|---|---|---|---|---|---|
| AST (U/L) | 103 ± 10.45 | 136.53 ± 19.94∗ | 117.88 ± 15.37 | 113.5 ± 7.7 | 98.85 ± 10.94# |
| ALT (U/L) | 40.5 ± 3.89 | 54.32 ± 4.76∗ | 54.05 ± 7.18 | 41.32 ± 6.25# | 34.68 ± 2.71# |
| Serum TG (nmol/L) | 0.4 ± 0.06 | 1.01 ± 0.12∗ | 1.09 ± 0.04 | 1.03 ± 0.05 | 0.82 ± 0.08# |
| Liver TG (mmol/g prot) | 0.07 ± 0.01 | 0.1 ± 0.02∗ | 0.09 ± 0.01 | 0.07 ± 0.01# | 0.06 ± 0.01# |
| Lipid peroxidation (nmol MDA equivalent/mg prot) | 0.64 ± 0.14 | 1.26 ± 0.22∗ | 0.88 ± 0.12# | 0.84 ± 0.15# | 0.72 ± 0.13# |
| SOD (U/mg prot) | 89.6 ± 3.42 | 97.51 ± 3.96∗ | 85.27 ± 5.57# | 83 ± 9.28# | 81.03 ± 6.65# |
| CAT (U/mg prot) | 6.55 ± 0.41 | 6.29 ± 0.39 | 5.55 ± 0.64# | 5.47 ± 0.28# | 5.17 ± 0.51# |
Note. Control: normal group; Model: alcohol group; LL: alcohol and low dose of lemon juice group; LM: alcohol and medium dose of lemon juice group; LH: alcohol and high dose of lemon juice group. ∗ means the levels of the parameters in the model group were significantly (p < 0.05) different from that of the control group. # means the levels of the parameters in the treatment group were significantly (p < 0.05) different from that of the model group.
3.5. Histopathological Evaluation
Histopathology assessment of the liver was carried out for all groups (Figure 5). There was no pathological abnormality observed in the liver of the control group with preserved cytoplasm and distinct nucleus as shown in Figure 5(a). In Figure 5(b), it was observed in the model group that ethanol induced necrosis changes and substantial small fat droplets changes in liver section. However, livers of mice in all lemon juice treated groups showed noticeable recovery from ethanol induced liver damage with fewer small fat droplets changes and hepatocytes necrosis features.

The photomicrographs of liver sections taken from mice. (a) Normal group; (b) alcohol group; (c) alcohol and low dose of lemon juice group; (d) alcohol and medium dose of lemon juice group; (e) alcohol and high dose of lemon juice group. Arrow indicates a condition of small fat droplets changes, and the circle indicates hepatocytes necrosis, which mainly occurs in alcohol model group.
3.6. The In Vitro Antioxidant Activity, Total Phenolic Contents (TPC), and Total Flavonoid Contents (TFC) of Lemon Juice
The in vitro antioxidant activities of lemon were evaluated using ferric-reducing antioxidant power (FRAP) and Trolox equivalent antioxidant capacity (TEAC) assays. The FRAP and TEAC values were 50.82 ± 2.70 μmol Fe(II)/g dry weight (DW) and 19.88 ± 0.66 μmol Trolox/g DW, respectively. The total phenolic contents (TPC) and total flavonoid contents (TFC) of lemon were 6.21 ± 0.28 mg GAE/g DW and 0.30 ± 0.03 mg QE/g DW, respectively.
4. Discussion
Alcohol use disorder causes substantial diseases, and the liver is the most adversely affected organ. In the present study, the effects of lemon juice on chronic alcohol-induced liver injury in mice were investigated. Ethanol induced impairment of liver in mice was evidenced by increased AST and ALT levels. Treatment with lemon juice lowered the increased levels of AST and ALT in serum. The return of the activities of aminotransferases (AST or ALT) in serum to normal indicates the regeneration of hepatocytes and the healing of hepatic parenchyma; therefore, lemon juice had a protective effect on alcohol-induced liver injury. The results were in agreement with previous reports that showed lemon possessing a hepatoprotective effect on liver injury induced by carbon tetrachloride and acute exercise [7, 13]. In addition, the chronic alcohol-induced liver damage was further confirmed by liver histopathological changes in the present study, and treatment with lemon juice also remarkably improved the liver histopathological changes, which further confirmed the hepatoprotective activity of lemon juice on alcohol-induced liver injury in mice.
Various factors and mechanisms are associated with the pathological progress of alcohol-induced liver injury, and oxidative stress was one of them [3]. ROS is one kind of prooxidants including hydroxyl radical, superoxide radical, and hydrogen peroxide, which are frequently generated spontaneously during metabolism. Normally produced ROS is rapidly eliminated by the antioxidant defense system. The antioxidant defense system is able to scavenge ROS and terminate chain reaction of free radicals in vivo. Alcoholic exposure can result in excessive accumulation of ROS and contribute to cellular damage. Excessive accumulation of ROS could cause lipid peroxidation of hepatocytes, which was regarded as the primary mechanism concerned with chronic alcohol-induced liver damage [8]. MDA, the product of lipid peroxidation induced by ROS, also accumulates in the alcohol-damaged liver and represents a good estimation of the total oxidative stress [3]. In the present study, alcohol significantly augmented lipid peroxidation levels, which was similar to the previous study that showed increased lipid peroxidation in alcoholic patients [14]. Treatment with lemon juice reduced the level of lipid peroxidation to a normal level, which showed a significant protective effect of lemon juice against alcohol-induced oxidative stress.
Liver steatosis is the earliest disease of the liver on account of chronic ethanol consumption, with the characteristic of fat accumulation. It is generally accepted that, in the development of hepatic steatosis, ethanol exposure increases the ratio of reduced nicotinamide adenine dinucleotide/oxidized nicotinamide adenine dinucleotide in hepatocytes, which disturb mitochondrial fatty acid β-oxidation and induce steatosis further [15]. In this study, alcohol-induced occurrence of hepatic steatosis was confirmed by increased hepatic TG contents and histopathological changes. Treatment with lemon juice significantly lowered the hepatic TG contents and improved the damaged histopathological changes. In particular, the mice given high dose of lemon juice had almost completely recovered to normal.
The antioxidant enzymes, such as SOD and CAT, represent the defense response system to excessive ROS. SOD catalyzes the dismutation of two superoxide anions to hydrogen peroxide and oxygen, and then CAT degrades two hydrogen peroxide molecules to water and oxygen [16]. SOD is also considered as front line among antioxidant enzymes in defense against free radicals. In the literature, the effects of alcohol treatment on the levels of SOD/CAT are controversial. SOD showed an increase, no changes, or a decrease, depending on the model, diet, duration, and amount of alcohol consumption [17–19]. In addition, it was reported that CAT activity decreased upon chronic ethanol consumption in a study [20]. However, another study showed that CAT activity was increased in rat liver [18]. In our study, the alcohol treatment significantly increased the activity of SOD and slightly decreased the activity of CAT, while treatment with lemon juice decreased the activities of SOD and CAT. The increased activity of SOD reflects the activation of the compensatory mechanism which might be an attempt to counteract free radicals in the liver [21]. The treatment with lemon juice prevented ROS accumulation, and the compensatory effects were not available in the liver. Therefore, lemon juice decreased the activities of SOD and CAT. The results were similar to the report of Gasparotto et al. [22]. In addition, the in vitro antioxidant experiment of lemon also showed that lemon had medium in vitro antioxidant capacities, which contribute to the explanation of the in vivo free radical scavenging effect of lemon.
Lemon contains numerous beneficial bioactive compositions, including phenolic compounds (mainly flavonoids), vitamins, carotenoids, essential oils, minerals, and dietary fiber [6]. The hepatoprotective effect of lemon may be attributable to the presence of vitamins, flavonoids, essential oils, and pectin. Vitamin C, a water-soluble antioxidant in lemon, is in a unique position to scavenge aqueous peroxyl radicals and react with free radicals, thus preventing oxidative damage including lipid peroxidation [14]. Sometimes, vitamin C could exert prooxidative effects at low concentrations and in the existence of transition metal ions [23], which might aggravate oxidative stress. However, it is difficult for vitamin C to have prooxidative effects in vivo due to the presence of NADPH-dependent recycling systems and glutathione [24]. In addition, there were some literatures reporting that vitamin C supplementation alone could reduce oxidative stress induced by ethanol, and the hepatoprotective effect of vitamin C treatment was more effective than silymarin, quercetin, and thiamine [25, 26]. Flavonoids, a class of secondary plant phenolics, can interact with hydroxyl radicals, chelate metal catalysts, and inhibit oxidases [27]. In previous studies, lemon flavonoid was shown to possess a hepatoprotective effect on liver damage induced by carbon tetrachloride and acute exercise, and the mechanism of the protective effect was related to the antioxidant capacity [7, 13]. Lemon essential oils and pectin were found to have protective effects on stomach and intestine barrier function [28, 29]. Ethanol exposure can injure the defensive intestinal barrier and increase the permeability of the small intestine, which lead to bacterial endotoxins leakage [25]. The bacterial endotoxins leakage is an important factor in the pathogenesis of alcohol-induced liver injury [30]. Therefore, the lemon essential oils and pectin might protect the intestine barrier function, thus indirectly protecting against alcohol-induced liver injury.
In this study, lemon juice revealed a protective effect on chronic alcohol-induced liver injury. Due to the fact that lemon contains a variety of bioactive ingredients, the hepatoprotective effect might be the result of joint action of multiple mechanisms, and it is difficult to clarify the specific mechanism of effect. The medium in vitro antioxidant capacities of lemon and reduced in vivo MDA levels indicated that lemon might reduce the oxidative stress induced by ethanol, thus exerting hepatoprotective effects. This study has found that lemon juice has a strong hepatoprotective effect, which provides valuable information for the general public to reduce harm of alcohol consumption. In the future, active components in lemon juice should be separated and identified, and the mechanism of action of the purified compound should be explored, including the action on the small intestine.
5. Conclusions
Chronic alcohol consumption could induce liver injury. Lemon juice is readily available as a widely consumed beverage. In this study, we found that treatment with lemon juice exerted hepatoprotective effects on alcohol-induced liver injury in mice through decreasing the levels of serum ALT and AST as well as hepatic TG and lipid peroxidation. In addition, the in vitro antioxidant experiment of lemon showed that lemon had medium in vitro antioxidant capacities. Therefore, we speculate that the hepatoprotective effects might be related to the antioxidant capacities of lemon juice. The results showed that lemon juice might be a potential dietary supplement for the prevention and treatment of liver injury related to chronic alcohol consumption.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (no. 81372976), Key Project of Guangdong Provincial Science and Technology Program (no. 2014B020205002), and the Hundred-Talents Scheme of Sun Yat-sen University.
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
Similar articles
-
The Treatment of Rheumatic Diseases by Lemon-Juice; with Illustrative Cases from Hospital Practice.
Br Foreign Med Chir Rev. 1849 Oct;4(8):529-530.PMID: 30164951 Free PMC article. Review. No abstract available. -
J Agric Food Chem. 2016 Sep 28;64(38):7291-7. doi: 10.1021/acs.jafc.6b02907. Epub 2016 Sep 19.PMID: 27609057
-
Int J Mol Sci. 2015 Jan 22;16(2):2446-57. doi: 10.3390/ijms16022446.PMID: 25622257 Free PMC article.
-
Food Funct. 2012 Jun;3(6):628-34. doi: 10.1039/c2fo10266h.PMID: 22648047
-
Protective effect of bicyclol on acute alcohol-induced liver injury in mice.
Eur J Pharmacol. 2008 May 31;586(1-3):322-31. doi: 10.1016/j.ejphar.2008.02.059. Epub 2008 Feb 29.PMID: 18371952
Cited by
-
Antioxidants (Basel). 2024 May 10;13(5):588. doi: 10.3390/antiox13050588.PMID: 38790693 Free PMC article.
-
Forensic Toxicol. 2024 Jan;42(1):45-59. doi: 10.1007/s11419-023-00674-w. Epub 2023 Oct 9.PMID: 37814103
-
Prevention of the Pro-Aggressive Effects of Ethanol-Intoxicated Mice by Schisandrin B.
Nutrients. 2023 Apr 15;15(8):1909. doi: 10.3390/nu15081909.PMID: 37111128 Free PMC article. -
Cells. 2022 Apr 12;11(8):1305. doi: 10.3390/cells11081305.PMID: 35455983 Free PMC article.
-
Nutrients. 2021 May 11;13(5):1612. doi: 10.3390/nu13051612.PMID: 34064981 Free PMC article. Review.
References
-
- Arteel G., Marsano L., Mendez C., Bentley F., McClain C. J. Advances in alcoholic liver disease. Best Practice and Research in Clinical Gastroenterology. 2003;17(4):625–647. – PubMed
Taraxacum official (dandelion) leaf extract alleviates high-fat diet-induced nonalcoholic fatty liver
Abstract
The purpose of this study is to determine the protective effect of Taraxacum official (dandelion) leaf extract (DLE) on high-fat-diet (HFD)-induced hepatic steatosis, and elucidate the molecular mechanisms behind its effects. To determine the hepatoprotective effect of DLE, we fed C57BL/6 mice with normal chow diet (NCD), high-fat diet (HFD), HFD supplemented with 2g/kg DLE DLE (DL), and HFD supplemented with 5 g/kg DLE (DH). We found that the HFD supplemented by DLE dramatically reduced hepatic lipid accumulation compared to HFD alone. Body and liver weights of the DL and DH groups were significantly lesser than those of the HFD group, and DLE supplementation dramatically suppressed triglyceride (TG), total cholesterol (TC), insulin, fasting glucose level in serum, and Homeostatic Model Assessment Insulin Resistance (HOMA-IR) induced by HFD. In addition, DLE treatment significantly increased activation of adenosine monophosphate (AMP)-activated protein kinase (AMPK) in liver and muscle protein. DLE significantly suppressed lipid accumulation in the liver, reduced insulin resistance, and lipid in HFD-fed C57BL/6 mice via the AMPK pathway. These results indicate that the DLE may represent a promising approach for the prevention and treatment of obesity-related nonalcoholic fatty liver disease.
Keywords: AMPK; Fatty liver; High-fat diet; Insulin resistance; Taraxacum official (dandelion).
Copyright © 2013 Elsevier Ltd. All rights reserved.
Similar articles
-
Dandelion (Taraxacum Genus): A Review of Chemical Constituents and Pharmacological Effects.
Molecules. 2023 Jun 27;28(13):5022. doi: 10.3390/molecules28135022.PMID: 37446683 Free PMC article. Review. -
Nutrients. 2022 Mar 24;14(7):1350. doi: 10.3390/nu14071350.PMID: 35405963 Free PMC article. Review.
-
Anti-obesity effects of Diospyros lotus leaf extract in mice with high-fat diet-induced obesity.
Int J Mol Med. 2019 Jan;43(1):603-613. doi: 10.3892/ijmm.2018.3941. Epub 2018 Oct 18.PMID: 30365061 -
Curcumin attenuates diet-induced hepatic steatosis by activating AMP-activated protein kinase.
Basic Clin Pharmacol Toxicol. 2013 Sep;113(3):152-7. doi: 10.1111/bcpt.12076. Epub 2013 May 25.PMID: 23574662 -
Cassia tora (Leguminosae) seed extract alleviates high-fat diet-induced nonalcoholic fatty liver.
Food Chem Toxicol. 2013 Jan;51:194-201. doi: 10.1016/j.fct.2012.09.024. Epub 2012 Sep 28.PMID: 23026700
Cited by
-
Foods. 2023 Oct 17;12(20):3800. doi: 10.3390/foods12203800.PMID: 37893693 Free PMC article.
-
Nutrients. 2023 Sep 24;15(19):4120. doi: 10.3390/nu15194120.PMID: 37836404 Free PMC article.
-
Dandelion (Taraxacum Genus): A Review of Chemical Constituents and Pharmacological Effects.
Molecules. 2023 Jun 27;28(13):5022. doi: 10.3390/molecules28135022.PMID: 37446683 Free PMC article. Review. -
Nutrients. 2022 Dec 24;15(1):80. doi: 10.3390/nu15010080.PMID: 36615741 Free PMC article.
-
Front Pharmacol. 2022 Sep 6;13:942996. doi: 10.3389/fphar.2022.942996. eCollection 2022.PMID: 36147318 Free PMC article.
- source
Protective Effects of Taraxacum officinale L. (Dandelion) Root Extract in Experimental Acute on Chronic Liver Failure
Abstract
Background: Taraxacum officinale (TO) or dandelion has been frequently used to prevent or treat different liver diseases because of its rich composition in phytochemicals with demonstrated effect against hepatic injuries. This study aimed to investigate the possible preventing effect of ethanolic TO root extract (TOERE) on a rat experimental acute on chronic liver failure (ACLF) model. Methods: Chronic liver failure (CLF) was induced by human serum albumin, and ACLF was induced in CLF by D-galactosamine and lipopolysaccharide (D-Gal-LPS). Five groups (n = 5) of male Wistar rats (200–250 g) were used: ACLF, ACLF-silymarin (200 mg/kg b.w./day), three ACLF-TO administered in three doses (200 mg, 100 mg, 50 mg/kg b.w./day). Results: The in vivo results showed that treatment with TOERE administered in three chosen doses before ACLF induction reduced serum liver injury markers (AST, ALT, ALP, GGT, total bilirubin), renal tests (creatinine, urea), and oxidative stress tests (TOS, OSI, MDA, NO, 3NT). Histopathologically, TOERE diminished the level of liver tissue injury and 3NT immunoexpression. Conclusions: This paper indicated oxidative stress reduction as possible mechanisms for the hepatoprotective effect of TOERE in ACLF and provided evidence for the preventive treatment.
1. Introduction
Liver diseases are one of the major health problems in the world and became a general health care problem due to the high morbidity rate. They are associated with several risk factors such as inadequate nutrition, metabolic diseases, viral infection, ethanol, and drug use. Liver injury may trigger the onset of liver failure, a common medical condition with very high mortality [1]. Liver failure can progress as acute liver failure (ALF), as acute on chronic liver failure (ACLF), or as acute decompensation of end-stage liver disease [2]. ALF is defined as a severe liver injury in the absence of pre-existing liver disease. According to the World Gastroenterology Organization ACLF is defined as “a syndrome in patients with chronic liver disease with or without previously diagnosed cirrhosis, characterized by acute hepatic decompensation resulting in liver failure (jaundice and prolongation of the international normalized ratio) and one or more extrahepatic organ failures, associated with increased mortality up to three months” [2,3]. The prevalence of ACLF ranges from 24% to 40%, and it usually occurs in young or middle-aged patients [4] and it is potentially reversible [2].
The exact mechanism of ACLF is not fully elucidated but based on what was found the pathophysiology was described using a four-stage model: precipitating event, hepatic injury due to precipitating event, response to injury, and failure of other organs [4,5]. The precipitating event can be triggered by one or more factors, identified or unidentified, like infections, alcohol, gastrointestinal bleeding, reactivation of viral hepatitis B (HBV), superinfection with hepatitis A or E virus, acute episodes of autoimmune hepatitis, Wilson’s disease, or vascular liver disease [2,6,7]. During the propagation phase, the number of proinflammatory mediators increases, a systemic inflammatory response syndrome and a vascular endothelial dysfunction will be activated, with progression to organs failure. At the same time, liver macrophages release anti-inflammatory cytokines that will initiate a compensatory anti-inflammatory response syndrome, leading to an acquired immunodeficiency, a “paralysis of the immune response” [4,8]. Measurement of oxidative stress, inflammation, necrosis, and apoptosis biomarkers can define the risk profile of ACLF [4,8]. The presence of multiple organ failure is a requirement for the diagnosis of ACLF, and the number of affected systems has a prognostic value. The kidneys are the most commonly affected organs [2,3].
Thus, the therapy for chronic hepatic diseases needs to develop new prophylactic agents to prevent ACLF. With the extended studies upon the use of medicinal plants, phytotherapy became an important support for the treatment of many diseases. The use of medicinal plants in the treatment of liver diseases has a long history worldwide because many phytochemicals have hepatoprotective activity [1,9,10]. Only a few of the ethnomedicinal effects have been scientifically validated [11]. Considering that in ACLF inflammation and oxidative stress are important pathogenetic mechanisms, the herbal medicines that have anti-inflammatory and antioxidant effects could be a promising source of bioactive compounds [12].
The Taraxacum officinale F. H. Wigg. (TO) (dandelion) species belong to the Asteraceae family, includes 30–57 varieties, and are widely distributed in the warm-temperate zones of the Northern Hemisphere [13,14,15]. It is a plant used in folk medicine from ancient times as anti-inflammatory, antioxidant, diuretic, choleretic, laxative, and hepatoprotective. Because the phytochemical components may define the medicinal value of a plant, their identification and effects mechanism in disease prevention and treatment is a necessity [11]. Furthermore, it has to be considered that the chemical composition of the TO extracts depends on both the extraction protocol and the solvents used (ethanol, acetone, water, or methanol) [16], but also on which part of the plant has been used (whole plant, roots, stem, leaves, flowers).
TO is also frequently used in different food products, and dietary supplements [17]. These plants were found to be rich in polyphenolic compounds, vitamins, inositol, lecithin, and minerals, and to exhibit antioxidant, anti-inflammatory, antiallergic, anti-hyperglycemic, hypolipidemic, and anticoagulant activities [9,18,19], to protect against hepatic injuries, but the mechanisms of action are still incompletely investigated [20].
It was demonstrated that TO root extract may protect against some toxic hepatic injury [11,13,21,22], but there are no studies on the potential hepatoprotective effect of this extract in ACLF. Therefore, our study aimed to extend the characterization of the ethanolic TO root extract (TOERE) and evaluate the potential use as a preventive hepatoprotective agent in a rat d-galactosamine and lipopolysaccharide (D-Gal-LPS)-induced rat ACLF model.
2. Materials and Methods
2.1. Chemicals
Phenolic compounds Sigma (St. Louis, MO, USA), Roth (Karlsruhe, Germany), Dalton (Toronto, ON, Canada); phytosterols Sigma (St. Louis, MO, USA); Folin–Ciocâlteu reagent, sulfanylamide (SULF), N- (1-Naphthyl) ethylenediamine dihydrochloric acid (NEDD), vanadium chloride (III) (VCl3), methanol, diethyl ether, xylenol orange [o-cresosulfonphthalein-3,3-bis (sodium methyliminodiacetate)], orthodianisidinedihydrochloric acid (3-3′-dimethoxybenzidine), ferrous ammonium sulfate, hydrogen peroxide (H2O2), sulfuric acid, hydrochloric acid, glycerol, trichloroacetic acid (TCA), ethylenediaminetetra-acetic acid, sodium dodecal, sulfate butylated hydroxytoluene, thiobarbituric acid, 1,1,3,3-tetraethoxypropane, 2,4-dinitrophenylhydrazine (DNPH), 5,5’-dithionitrobis 2-nitrobenzoic acid (DTNB), 1,1-diphenyl-2-picrilhydrazyl (DPPH), o-phthalaldehyde Merck (Darmstadt, Germany); Trolox (6-hydroxy-2,5,7,8-tetramethylchroman-2-carboxylic acid) Alfa-Aesar (Karlsruhe, Germany); Freund’s adjuvant, d-galactosamine (D-Gal) and lipopolysaccharide (LPS) from Merck and Sigma-Aldrich (Taufkirchen, Germany); Human serum albumin (HSA) (Octapharma GmbH, Austria). All chemicals were of analytical grade. Aspartate aminotransferase, alanine aminotransferase, total bilirubin, alkaline phosphatase, gamma glutamate transferase, creatinine, and urea kits were purchased from Spinreact (Sant Esteve de Bas, Spain). ELISA kit for 3-nitrotyrosine (KA0445-ABNOVA EMBLEM, Heidelberg, Germany) and primary antibody to 3-Nitrotyrosine for immunohistochemistry (Code ALX-804-505-C050, Enzo Life Sciences) were also used.
2.2. Plant Material
Fresh T. officinale F.H. Wigg. roots from the Alexandru Borza Botanical Garden “Babes-Bolyai” University of Cluj-Napoca, Romania, were purchased in June 2020, deposited in “Alexandru Borza” Botanical Garden Herbarium (Voucher CL:669002), and plant extract was prepared as previously described [23]. The roots were dried in a shaded place, grounded in a coffee grinder (Argis, RC-21, Electroarges SA, Curtea de Arges, Romania) for 5 min, and then the powder was screened through a 200 μm Retsch sieve [24]. Fifty grams were weighed and extracted with 70% ethanol, twice for 30 min using the UltraTurrax extraction apparatus (T 18; IKA Labortechnik, Staufen, Germany) at room temperature. The samples were then centrifuged at 4000 rpm for 30 min, and the supernatant was recovered, and filtered through a 0.45 μm micropore membrane (PTFE, Waters, Milford, MA, USA). The solvent was evaporated at 40 °C using a rotary evaporator (Hei-VAP, Heidolph Instruments GmbH & Co., Schwabach, Germany). Further, the obtained extracts were lyophilized (Advantage 2.0, SP Scientific, Warminster, PA, USA) [24]. The extract powder was stored at room temperature in airtight bottles. The extraction yield was 15.2% (w/w).
2.3. Phytochemical Analysis
Identification and Quantification of Polyphenolic Compounds by HPLC-DAD-ESI MS
The phenolic compounds of the T. officinale extracts were determined as previously described [23,24] with some modifications. Prior to LC analysis, the lyophilized extract was dissolved in MeOH. Chlorogenic acid was used for phenolic acid quantification, and results were expressed as mg chlorogenic acid equiv./g of dry plant material (mg CA/g d.w.) [25].
2.4. Animals and Experimental Design
The experiments were carried out on adult male Albino Wistar rats (strain Crl: WI), weighing 200–250 g, bred in the Animal Facility of Iuliu Hațieganu University of Medicine and Pharmacy, Cluj-Napoca as previously described [23]. Animals were randomly divided into 6 groups (n = 5): Control group with no disease and no treatment, acute on chronic liver failure (ACLF) group, ACLF with Silymarin pretreatment (ACLF-SYL) group (200 mg/kg b.w./day) [26], ACLF groups with TOERE pretreatment in three doses, respectively ACLF-TO200 (200 mg dry plant material/kg b.w./day), ACLF–TO100 (100 mg dry plant material/kg b.w./day), and ACLF-TO50 (50mg dry plant material/kg b.w./day). The daily dose of TOERE has been dissolved in corn oil (1ml/day/animal). All the procedures performed on laboratory animals, comply with the Directive 2010/63/EU, and Romanian national law 43/2014 for animal protection used for scientific purposes. The project was approved by the Veterinary Sanitary Direction and Food Safety Cluj-Napoca as previously described (no. 19/ 13.12.2016) [23].
The ACLF rat model was induced by human serum albumin (HSA), d-galactosamine (D-Gal), and lipopolysaccharide (LPS) as previously described [27,28]. Silymarin (SYL) or TO have been administrated per os (p.o.) by gavage for 7 days. The ACLF group was pretreated for 7 days with physiological saline (1 mL/day/animal). After completing the treatments, on day 8 in the ACLF, ACLF-TO200, ACLF-TO100, ACLF–TO50, and ACLF-SYL groups ACLF was induced by the intraperitoneal injection (i.p.) of d-galactosamine (D-Gal) (400 mg/kg b.w.) and lipopolysaccharide (LPS) (100 μg/kg b.w.) [27,29]. Six hours after ACLF induction the rats were anesthetized with ketamine (60 mg/kg b.w.) and xylazine (15 mg/kg b.w.), blood was withdrawn by retro-orbital puncture, serum was separated by centrifugation, and stored at −80 °C until use. At the end of the experiment, under general anesthesia animals were killed by cervical dislocation and liver biopsy was harvested from each animal. The experiments were performed in triplicate.
2.5. Biochemical Serum Analysis
The hepatic injury was evaluated with conventional serum liver markers: serum aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin (BT), alkaline phosphatase (ALP), and gamma glutamate transferase (GGT) as previously described [23]. Oxidative stress associated with liver injury was evaluated by measuring serum total oxidative status (TOS), total antioxidant reactivity (TAR), oxidative stress index (OSI), malondialdehyde (MDA), total thiols (SH), total nitrites, and nitrates (NOx) and 3-nitrotyrosine (3NT) levels as previously described [23,30,31]. Renal failure induced by ACLF was diagnosed with creatinine and urea.
2.6. Histological Assessment
For the histological analysis two liver fragments were collected from the left lateral and right medial lobes [32], fixed in 10% phosphate-buffered formalin for 24 h, and routinely processed and embedded in paraffin wax. From each tissue fragment, two serial sections of 3 µm were stained with hematoxylin and eosin (H&E). The hepatic parenchyma was histologically assessed for intralobular and periportal degeneration/necrosis, portal inflammation, and fibrosis, and the Histological Activity Index (HAI) was calculated [33,34].
2.7. Immunohistochemical Analysis of 3-Nitrotyrosine
For the immunohistochemical analysis of 3NT, the paraffin sections were dewaxed in xylene, followed by rehydration in decreasing the concentration of alcohol. Sodium citrate buffer (pH = 6) was used for epitope retrieval and endogenous peroxidase was blocked with peroxidase for 5 min. The primary mouse monoclonal [clone 39B6] antibody to 3NT was diluted in 1% PBS-BSA (bovine serum albumin) at 1:200, and maintained overnight at 4 °C in a humid chamber, followed by placing the secondary antibody. The reaction was visualized using 3,3’-diaminobenzidine. Finally, the sections were counterstained with Mayer’s hematoxylin. The positive reaction was given by the brown labeling of the hepatocytes. Immunopositivity for 3NT was evaluated and scored, as follows: grade 0, no staining; grade 1, positive staining in less than 10% of hepatocytes/10 high power fields; grade 2, positive staining in more than 10% but less than 50% of hepatocytes/10 high power fields; grade 3, positive staining of more than 50% of hepatocytes/10 high power fields [35].
The sections were independently examined by two pathologists (MT and CT) using a light Olympus BX-41 microscope, and a multi-head microscope Zeiss Axio Scope A1 (Carl Zeiss Microscopy GmbH, Germany). When there was a divergence of opinion, an agreed diagnosis was reached by a simultaneous evaluation in a multi-head microscope Zeiss Axio Scope A1 (Carl Zeiss Microscopy GmbH, Germany). The photomicrographs were taken using an Olympus SP 350 digital camera and Stream Basic imaging software (Olympus Corporation, Tokyo, Japan).
2.8. Statistical Analysis
All results were expressed as mean ± standard deviation (SD) whenever data were normally distributed. Comparisons between the different experimental groups were performed using the one-way ANOVA test and the post hoc Bonferroni–Holm test. The correlations analysis was performed with the Pearson test. Values of p < 0.05 were considered statistically significant. The analysis was performed using IBM SPSS Statistics, version 20 (SPSS Inc. Chicago, IL, USA).
3. Results
3.1. Phytochemical Analysis
In our study, HPLC-DAD-ESI MS identified significant concentrations of hydroxybenzoic, caffeic, and chicoric acids (Figure 1, Table 1).

Table 1
Identification and quantification of Taraxacum officinale root extract polyphenols from hydroxybenzoic and hydroxycinnamic acids groups.
| No | Retention Time Rt (min) |
UV λmax (nm) |
[M+H]+ (m/z) |
Tentative Identification | Concentration * mg CA/ g TOERE |
|---|---|---|---|---|---|
| 1 | 2.95 | 270 | 138 | Hydroxybenzoic acid | 3.65 ± 0.15 |
| 2 | 13.62 | 320 | 181, 163 | Caffeic acid | 1.09 ± 0.02 |
| 3 | 14.19 | 322 | 475, 312 | Chicoric acid | 1.95 ± 0.15 |
| 4 | 15.50 | 322 | 369 | Feruloylquinic acid | 0.6 ± 0.08 |
| 5 | 19.93 | 322 | 516, 181,163 | Dicaffeoylquinic acid | 0.53 ± 0.04 |
| 6 | 20.12 | 322 | 516, 181,163 | Dicaffeoylquinic acid isomer | 0.4 ± 0.03 |
* mg CA/g TOERE-chlorogenic acid equiv. mg/g Taraxacum officinale ethanolic root extract. Values are the mean ± SD (n = 3).
3.2. Biochemical Serum Analysis
The hepatic injury was evaluated by measuring liver markers (AST, ALT, ALP, GGT, TB) [36] (Table 2). ACLF induction by D-Gal-LPS caused a severe increase of the liver markers than in Control animals (p < 0.001). Administration for a week of three different doses of TOERE or SYL in ACLF animals significantly prevented severe ACLF-induced increase of the AST, ALT, ALP, GGT, and TB (p < 0.001). Furthermore, the TOERE effect was dose-dependent, with the 100 mg TOERE/kg b.w./day concentration having the best inhibitory effect. In ACLF-TO200 and ACLF-TO100 groups TOERE hepatoprotective effects were better than in ACLF-SYL animals (p < 0.01) (Table 2).
Table 2
Liver and renal screening tests of the study groups.
| Groups | AST (U/L) | ALT (U/L) | TB (mg/dL) | ALP (mg/dL) | GGT (mg/dL) | Urea (mg/dL) | CR (mg/dL) |
|---|---|---|---|---|---|---|---|
| ACLF-TO200 | 81.12 a ± 5.27 | 71.64 a,b,c ± 11.32 | 2.27 a,b,c ± 0.37 | 328.45 a,b ± 14.72 | 60.42 a,b,c ± 9.20 | 67.14 a,b,c ± 4.21 | 1.75 a,b ± 0.21 |
| ACLF-TO100 | 82.14 a,b,c ± 4.20 | 54.08 b,c ± 12.37 | 1.30 b,c ± 0.27 | 310.38 a,b,c ± 11.19 | 49.97 b,c ± 8.37 | 78.93 a,b ± 5.18 | 1.78 a,b ± 0.14 |
| ACLF-TO50 | 84.24 a,b,c ± 8.06 | 144.93 a,b,c ± 19.79 | 2.02 a,b ± 0.51 | 329.61 a,b ± 37.89 | 107.34 a,b,c ± 18.33 | 110.30 a,b,c ± 7.89 | 2.15 a,b ± 0.40 |
| ACLF-SYL | 126.37 a,b ± 6.58 | 111.67 a,b ± 13.04 | 2.44 a,b ± 0.13 | 332.59 a ± 29.20 | 74.51 a,b ± 9.86 | 81.25 a,b ± 12.15 | 2.02 a,b ± 0.29 |
| ACLF | 222.65 a,c ± 11.08 | 174.08 a,c ± 15.16 | 3.74 a,c ± 0.53 | 358.94 a,c ± 13.55 | 117.71 a,c ± 15.47 | 255.49 a,c ± 19.48 | 3.53 a,c ± 0.28 |
| Control | 35.04 ± 6.63 | 47.55 ± 10.08 | 1.01 ± 0.11 | 263.75 ± 15.20 | 44.31 ± 4.58 | 39.16 ± 2.71 | 0.57 ± 0.04 |
Results are expressed as mean ± SD. Values are expressed as mean ± SD (n = 5). a p ˂ 0.05, versus Control; b p ˂ 0.05, versus ACLF; c p ˂ 0.05, versus SYL. AST—aspartate aminotransferase; ALT—alanine aminotransferase; TB—total bilirubin; ALP—alkaline phosphatase; GGT—gamma-glutamyltransferase; CR—creatinine; ACLF-TO200- acute on chronic liver failure pretreated with 200 mg TOERE/kg b.w./day; ACLF-TO100—acute on chronic liver failure pretreated with 100mg TOERE/kg b.w./day; ACLF-TO50—acute on chronic liver failure pretreated with 50 mg TOERE/kg b.w./day; ACLF-SYL—acute on chronic liver failure pretreated with 200 mg silymarin/kg b.w./d; ACLF—acute on chronic liver failure; Control—negative control.
Considering that in ACLF kidneys are the most affected organs, in a study of a plant with possible hepatoprotective use in ACLF it is also important to determine the nephroprotective activity. ACLF induction by D-Gal- LPS caused a severe increase of creatinine and urea (p < 0.001). Renal dysfunction tests were positively correlated with the liver markers (r = 0.6–0.9) in ACLF animals. The treatments of ACLF rats with TOERE or SYL caused a smaller increase of serum creatinine and urea after ACLF induction (p < 0.001). SYL effect was comparable to that from ACLF-TO200 and ACLF-TO100 groups, but better than that from ACLF-TO50 animals (Table 2).
In our study systemic oxidative stress was also evaluated. Compared to the control, serum TOS, OSI, and MDA were elevated in ACLF animals (p < 0.001. The treatment with TOERE or SYL reduced TOS, OSI and MDA increase after ACLF induction (p < 0.01). TOERE effect on the oxidative stress was dose-dependent, the higher concentration having the best antioxidant effect (Table 3).
Table 3
Oxidative stress tests of the study groups.
| Groups | TOS (µM H2O2/L) |
TAR (mM TROLOX/L) |
OSI | MDA (nM/L) |
NOx (µM/L) |
3NT (nmol/L) |
SH (mM GSH/L) |
|---|---|---|---|---|---|---|---|
| ACLF-TO200 | 30.61 a,b,c ± 6.85 | 1.088 ± 0.001 | 31.57 a,b,c ± 6.13 | 3.05 a,b,c ± 0.28 | 21.92 b,c ± 3.74 | 769.36 a,b,c ± 78.46 | 0.48 a,b ± 0.03 |
| ACLF-TO100 | 35.50 a,b,c ± 7.27 | 1.089 ± 0.001 | 31.17 a,b,c ± 4.84 | 3.67 b ± 0.59 | 25.76 a,b,c ± 4.50 | 768.66 a,b,c ± 69.75 | 0.48 a,b ± 0.08 |
| ACLF-TO50 | 40.45 a,b,c ± 8.46 | 1.089 ± 0.001 | 31.82 a,b,c ± 9.39 | 3.95 a,b ± 0.47 | 30.52 a,b,c ± 7.60 | 820.20 a,b,c ± 48.43 | 0.48 a,b ± 0.02 |
| ACLF-SYL | 36.41 a,b ± 7.75 | 1.092 ± 0.003 | 37.03 a,b ± 8.27 | 3.83 a,b ± 0.34 | 36.56 a,b ± 6.76 | 971.07 a,b ± 68.34 | 0.52 a,b ± 0.02 |
| ACLF | 47.98 a,c ± 7.95 | 1.089 ± 0.001 | 40.40 a,c ± 8.60 | 5.37 a,c ± 0.08 | 51.49 a,c ± 7.32 | 1053.99 a,c ± 91.15 | 0.40 a,c ± 0.03 |
| Control | 21.18 ± 1.72 | 1.089 ± 0.001 | 21.59 ± 4.61 | 3.57 ± 0.36 | 19.98 ± 1.99 | 480.45 ± 56.62 | 0.59 ± 0.01 |
Results are expressed as mean ± SD. a p ˂ 0.05, versus Control; b p ˂ 0.05, versus ACLF; c p ˂ 0.05, versus SYL. TOS—total oxidative status; TAR—total antioxidant reactivity; OSI—oxidative stress index; NOx—nitric oxide; 3NT—3-nitrotyrosine; MDA—malondialdehyde; SH—total thiols; ACLF-TO200—acute on chronic liver failure pretreated with 200 mg TOERE/kg b.w./day; ACLF-TO100—acute on chronic liver failure pretreated with 100 mg TOERE/kg b.w./day; ACLF-TO50—acute on chronic liver failure pretreated with 50 mg TOERE/kg b.w./day; ACLF-SYL—acute on chronic liver failure pretreated with 200 mg silymarin/kg b.w./d; ACLFacute on chronic liver failure; Control—negative control.
In ACLF rats NOx and 3NT were also increased (p < 0.001). TOERE pretreatments prevented NOx and 3NT elevation (p < 0.001) after ACLF induction in a dose-dependent way, with a higher concentration having a better inhibitory activity. SYL was also a good inhibitor of NO production and peroxidation in ACLF animals (p < 0.001), but the effect was smaller than that of TOERE (Table 3).
Additionally, serum antioxidative activity was evaluated by measuring TAR and SH. TAR was not influenced by ACLF induction (p > 0.05). A depletion in the level of SH was observed in ACLF rats (p < 0.01), and the treatment with TO or SYL prevent SH reduction (p < 0.05) after ACLF induction. SYL has a better effect than TO on SH (Table 3).
3.3. Histological Assessment
In the livers of the Control group, no significant structural changes were observed (Figure 2a).

Photomicrographs of the liver tissues from the control and experimental animals. H&E stain: (a). Control; (b). ACLF; (c). ACLF-SYL; (d). ACLF-TO200; (e). ACLF-TO100; (f). ACLF-TO50; Bar = 50 µm (a–c,f) and 20 µm (d,e). ACLF—acute on chronic liver failure; ACLF-SYL—acute on chronic liver failure pretreated with 200 mg silymarin/kg b.w./d; ACLF-TO200—acute on chronic liver failure pretreated with 200 mg TOERE/kg b.w./day; ACLF-TO100—acute on chronic liver failure pretreated with 100 mg TOERE/kg b.w./day; ACLF-TO50—acute on chronic liver failure pretreated with 50 mg TOERE/kg b.w./day.
The highest histological scores were identified in the livers of the ACLF group (p < 0.001) (Table 4). The changes were represented by congestion, hemorrhages, multifocal to coalescing areas of coagulative necrosis, randomly distributed within the hepatic lobules or centered on periportal regions and associated with severe and mixed inflammatory infiltrates. The portal spaces were also affected and expanded by fibrosis, bile duct hyperplasia, and large numbers of inflammatory cells, predominated by small lymphocytes and macrophages (Figure 2b). The microscopical examination of the livers from the group ACLF-SYL group (Figure 2c) revealed the lowest histological scores if compared to ACLF, ACLF-TO200, ACLF-TO100, and ACLF-TO50 (p < 0,001). Compared to the untreated ACLF group, in ACLF-TO200 (Figure 2d), ACLF-TO100 (Figure 2e), and ACLF-TO50 (Figure 2f) animals, the hepatic injuries were significantly reduced by the TOERE pretreatments (p < 0.001), with no important differences between different TOERE doses (p > 0.05). Liver necroinflammatory scores and serum liver tests were positively correlated.
Table 4
Histological and IHC scores of the liver biopsies.
| Groups | Portal Inflammation | Periportal Degeneration/ Necrosis |
Intralobular Degeneration/ Necrosis |
Fibrosis | HAI | 3NT |
|---|---|---|---|---|---|---|
| ACLF-TO200 | 1.60 a,b,c ± 0.89 | 2.20 a,b,c ± 0.10 | 1.00 a,b,c ± 0.01 | 1.20 a,c ± 0.10 | 5.80 a,c ± 1.92 | 1.40 a,b,c ± 0.55 |
| ACLF-TO100 | 2.20 a,b,c ± 0.10 | 2.60 a,b,c ± 0.89 | 1.40 a,b,c ± 0.89 | 1.00 a,c ± 0.10 | 7.20 a,b,c ± 1.10 | 1.40 a,b,c ± 0.55 |
| ACLF-TO50 | 2.60 a,b,c ± 0.89 | 2.20 a,b,c ± 1.10 | 2.20 a,b,c ± 1.10 | 1.00 a,c ± 0.10 | 8.00 a,b,c ± 1.41 | 1.80 a,b,c ± 0.45 |
| ACLF-SYL | 1.00 a,b ± 0.00 | 0.60 a,b ± 0.55 | 0.80 a,b ± 0.45 | 0.40 a,b ± 0.55 | 2.80 a,b ± 0.45 | 1.20 a,b ± 0.45 |
| ACLF | 3.60 a,c ± 0.55 | 4.80 a,c ± 0.84 | 3.60 a,b ± 0.55 | 1.00 a,b ± 0.10 | 12.80 a,b ± 1.64 | 2.40 a,b ± 0.55 |
| Control | 0.40 ± 0.55 | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.20 ± 0.45 | 0.00 ± 0.00 |
Results are expressed as mean ± SD. a p ˂ 0.05, versus Control; b p ˂ 0.05, versus ACLF; c p ˂ 0.05, versus SYL; ACLF-TO200—acute on chronic liver failure pretreated with 200 mg TOERE/kg b.w./day; ACLF-TO100—acute on chronic liver failure pretreated with 100mg TOERE/kg b.w./day; ACLF-TO50—acute on chronic liver failure pretreated with 50 mg TOERE/kg b.w./day; ACLF-SYL—acute on chronic liver failure pretreated with 200 mg silymarin/kg b.w./d; ACLF—acute on chronic liver failure; Control—negative control; HAI—histological activity index; 3NT—3-nitrotyrosine.
3.4. 3-Nitrityrosine Evaluation
3-NT immunoexpression was negative in the livers of the control group (Figure 3a). A marked hepatocellular immunoexpression of 3-NT with a diffuse or mediolobular pattern was found in all liver samples from the ACLF group (Figure 3b) (p < 0.01). In the group ACLF-SYL, the 3-NT expression was reduced compared to the ACLF group (p < 0.01), being mainly limited to hepatocytes near the portal spaces (Figure 3c) (Table 4).

Immunohistochemical expression of 3-nitrotyrosine (3-NT) in liver tissues from the control and experimental animals: (a). Control; (b). ACLF; (c). ACLF-SYL; (d). ACLF-TO200; (e). ACLF-TO100; (f). ACLF-TO50; Bar = 50 μm (a) and 20 μm (b–f). ACLF-TO200—acute on chronic liver failure pretreated with 200 mg TOERE/kg b.w./day; ACLF-TO100—acute on chronic liver failure pretreated with 100 mg TOERE/kg b.w./day; ACLF-TO50—acute on chronic liver failure pretreated with 50 mg TOERE/kg b.w./day; ACLF-SYL—acute on chronic liver failure pretreated with 200 mg silymarin/kg b.w./d.
As compared to the ACLF group, the expression of 3NT was lower in liver biopsies from TOERE treated animals, particularly in the ACLF-TO200 (Figure 3d) and ACLF-TO100 (Figure 3e) (p < 0.01) groups. The expression of 3NT in the ACLF-TO50 group (Figure 3f) was higher compared to the other treated groups. SYL effect on 3NT expression was better than that of TOERE (p < 0.05) (Table 4).
The correlation between the histological scores and biochemical tests were also analyzed. In ACLF, ACLF-TO200, ACLF-TO100, ACLF-TO50, and ACLF-SYL groups all histopathological scores were positively correlated with liver, renal, and oxidative stress markers.
4. Discussion
In the current study, D-Gal-LPS-induced ACLF in rats with HAS-induced chronic liver failure triggered an immune-mediated liver injury with pathological serum liver marker tests and histological liver changes. The liver injuries were also associated with renal failure and systemic oxidative stress. A seven days pretreatment with TOERE reduced ACLF induced liver injury. The protecting effect of TOERE can be attributed, at least in part, to the reduction of the oxidative stress associated with immune liver injury in D-Gal-LPS-induced ACLF. Depending on the dose, the hepatoprotective effect of TOERE was similar or lower than that of SYL, an already used hepatoprotective drug.
By analyzing the TOERE extract, other studies identified sesquiterpenes, various triterpenes, phenolic compounds, and phytosterols. Our previous phytochemical analysis [23] showed that the tested TO root extract had a lower TPC than in Aremu et al.’s analysis of TO root extract (1.14 ± 0.01 mg/100 GAE/mg extract) and TO leaf extract (4.35 ± 0.15 mg GAE/mg extract) [37], but higher than in the TO aerial part extract (15.50 mg GAE/g d.w.) [38].
The HPLC-DAD-ESI MS analysis of our TO root extract identified, caffeic acid, chicoric acid, as previously described [23], plus feruloylquinic acid, dicaffeoylquinic acid, and dicaffeoylquinic acid isomer. All these compounds have anti-inflammatory and antioxidant properties [11,23,39,40,41]. The antioxidant activity of the TOERE measured by DPPH and FRAP tests was proved in our previous study [23].
Because the chemical composition correlates with the pharmacological effects, TO extracts from different plant parts had different activities. Several studies demonstrated that the TO roots extract reduces alcohol-induced oxidative stress, TO leaf extract alleviates high-fat diet-induced nonalcoholic fatty liver, and TO flower extract can scavenge reactive oxygen species [22]. Similar to other studies [16,42,43], and based on the evidence of the phytochemical analysis results, our TO root extract can be considered a good natural antioxidant candidate. These results encouraged us to continue by testing the in vivo hepatoprotective and antioxidant effects of TOERE in an experimental ACLF.
For ACLF experimental model, first HAS administration in rats caused an immune liver injury and fibrosis, and then LPS stimulated liver macrophages leading to hepatic necro-inflammatory change. D-Gal, an amino sugar metabolized selectively by the hepatocytes, in a few hours potentiated the hepatotoxic effect of LPS by inhibiting mRNA and protein synthesis, leading to acute hepatitis [28]. The hepatoprotective effect of the TOERE was evaluated by using serum liver markers and liver histological analysis [2,3]. AST and ALT elevation reflects generalized damage to hepatocytes, TB increase reflects liver metabolism, ALP and GGT elevation reflects cholestasis [20,43,44]. In ACLF rats, liver markers were consistent with hepatocytes injury, cholestasis and, lower liver metabolism, demonstrating that an ACLF model was successfully induced [27]. The preliminary tests evaluating the TOERE effect on negative control animals indicated that the product had no significant activity on the healthy liver and oxidative stress (see supplemental data). In ACLF TO pretreatment reduced liver markers, suggesting that TOERE may prevent severe ACLF and by that to reduce the mortality due to ACLF. ACLF-TO100 group had the best hepatoprotective effect. In a previous study, we also evaluated in the TO root extract some phytosterols with anti-inflammatory and antioxidative properties [23]. It was demonstrated that due to their structural similarity with cholesterol, phytosterols are prone to be oxidized and transformed into oxyphytosterols [45,46,47], and from antioxidants to become pro-oxidants. By lowering the dose of TO from 200 to 100mg dry plant material/kg b.w./day, phytosterol reduction may be involved in the better hepatoprotective effect of ACLF-TO100 than of ACLF-TO200.
Liver injury diagnosed by serum liver tests was further confirmed by histopathological characteristics. In a normal liver, there is a hypoimmune response, and in chronic liver inflammation there is a high cellular recruitment, extended tissue damage, and the repair process leads to tissue remodeling, fibrosis, and liver dysfunction [41,48,49]. Fibrosis represents a key characteristic of progression towards liver cirrhosis and hepatic failure. In the present work liver biopsy of the ACLF animals showed extended necro-inflammatory changes, fibrosis, and bile ducts hyperplasia. In ACLF rats, like previously observed, histopathological scores increased due to the ongoing inflammation activation and the direct cytotoxic effect of cell death products [50]. Pretreatment with our TOERE in ACLF had hepatoprotective activity by reducing liver necro-inflammatory changes, with no important effect on liver fibrosis.
Under physiological conditions, free radicals are scavenged by antioxidant mechanisms. If there is an excess of free radicals or if there is a deficiency of antioxidants, oxidative stress will build up and will cause oxidative damage of lipids, proteins, and DNA [2,43,49]. In D-Gal-LPS-induced ACLF, immune-induced liver injury triggered an important liver inflammatory response and systemic oxidative stress, with high serum TOS and OSI, along with increased production of MDA, NOx, and 3NT.
Many studies correlated the hepatoprotective activity of the medicinal plant extracts with the antioxidant compounds from these plants [51]. Moreover, other experimental studies demonstrated that the polyphenolic compounds isolated from TO extracts had a hepatoprotective effect by reducing oxidative stress through direct free radical scavenging activity, metal ions chelation, and regeneration of the membrane-bound antioxidants [40,49]. In the present work, TOERE decreased serum TOS, OSI, and MDA levels in a dose-dependent way. MDA reduction was relevant because recently lipid peroxidation was considered a vital process in chronic liver diseases [44]. TOERE did not affect TAR, and SH was just slightly increased, indicating that this extract reduced systemic oxidative stress mainly by scavenging the oxidants and less by increasing the antioxidant capacity.
In mammals there are three NO synthase (NOS) isoenzymes that are involved in NO synthesis: neuronal (nNOS/NOS-1), inducible (iNOS/NOS-2), and endothelial (eNOS/NOS-3). Inflammatory stimuli up-regulate iNOS, and excessively generate NO induces nitrosative and oxidative damage. In liver injury, NO can be produced by hepatocytes, Kupffer cells, hepatic stellate cells (HSCs), and hepatic sinusoidal endothelial cells. It was observed that NO may have a dichotomous effect on liver disease, respectively in chronic liver diseases NO can promote HSC apoptosis, but in acute liver diseases, NO may increase liver damage. In LPS-treated rats, the marked hepatocellular immunoexpression of 3NT indicated that the iNOS-ROS cycle augments liver injury [52]. In this study, we found that liver 3NT was down-regulated following treatment with TOERE, suggesting that TOERE may reduce liver inflammatory responses and oxidative stress by reducing NO production through the inhibition of iNOS gene expression. These properties of TOERE may be explained by the high content of antioxidant phytochemicals.
Only iNOS and eNOS were highly expressed in acute liver failure (ALF) liver tissue, causing plasma NO elevation, and in humans increased plasma NO levels were correlated to the clinical severity of ALF [52]. In D-Gal-LPS-induced ACLF elevation of serum NOx and 3NT confirmed excessive NO synthesis due to the severe liver injury and inflammation. The treatment with TOERE reduced the serum NOx and 3NT, indirectly indicating that TOERE had a significant inhibitory effect on systemic NO production.
Because systemic oxidative stress markers reduction was correlated with serum liver markers and liver histopathological scores improvement, we concluded that TOERE lowered liver injury by reducing oxidative stress. Like in other studies [10], it was found that the antioxidant effect of TOERE was dose-dependent, the higher extract concentration had better antioxidant activity due to the high concentration of antioxidant ingredients.
According to the World Gastroenterology Organization ACLF is characterized by acute liver failure and one or more extrahepatic organ failure because in ACLF liver inflammation may trigger systemic inflammation. The kidneys are the most commonly affected organs and renal failure range from acute kidney injury (AKI) to acute-on-chronic kidney failure [2,3]. Therefore, acute kidney injury (AKI) was tested as a major criterion in ACLF severity grading [53]. In ACLF two subgroups of secondary renal dysfunctions with different pathophysiology and prognosis can be associated. One is the hepatorenal syndrome-acute kidney injury (HRS-AKI), a reduction of kidney function without parenchymal damage caused by prerenal insults such as hypovolemia. The other one is the non–HRS-AKI, induced by a renal insult such as inflammatory tubular injury in sepsis, bile acid nephropathy, and drug-induced tubular damage [54]. In ACLF liver protein synthesis lowers and may cause complications like coagulopathy, hemodynamic instability, jaundice, hepatic encephalopathy, hepatorenal syndrome, and sepsis [50]. At the same time, the systemic inflammatory response may also cause an inflammatory kidney injury with anon–HRS-AKI. Moreover, in experimental ACLF proinflammatory cytokines and LPS can cause directly renal tubular injury with cell apoptosis. Intrahepatic cholestasis from ACLF with increased serum bilirubin and bile acids may induce renal injury due to the direct renal toxicity and by tubular obstruction [54]. In our study, in ACLF animals creatinine and urea reached AKI levels, and there was a positive correlation between serum creatinine and urea, liver biopsy scores, and serum liver test. TOERE and SYL pretreatments reduced serum creatinine and urea in a dose-dependent way, indicating that in ACLF animals TOERE hepatoprotective activity is associated with a nephroprotective effect.
Lately, SYL has been used as a hepatoprotective agent due to its antioxidant and anti-inflammatory effects [55]. A finding of the study was that in experimental ACLF TO roots extract effects on serum liver markers were better than those of SYL, and SYL caused a higher reduction of the liver histological scores and 3NT immunoexpression. These differences suggested that TOERE better prevented acute liver injury and SYL reduces more the chronic response to liver injury. Even when SYL can reduce oxidative stress by scavenging ROS, by inhibiting ROS production [56], and by activating antioxidant enzymes [55], in our study it had a lower systemic antioxidant activity than TOERE.
5. Conclusions
This report highlights the hepatoprotective and nephroprotective effects of an ethanolic TO root extract on D-Gal-LPS-induced ACLF. The mechanism proposed is the antioxidant activity of the bioactive components of the TOERE. These findings suggest for the first time that TOERE may be a potential preventive therapeutic agent for the severe liver and renal inflammatory injury associated with ACLF. These observations are important considering that ACLF has a high mortality rate. Further studies and clinical trials are required to fully elucidate the beneficial effects of TO root extract supplementation to prevent ACLF.
Author Contributions
Conceptualization, I.O.P. and A.E.P.; methodology, T.A., R.M.P., L.V., and A.U.; software, R.M.P. and A.U.; validation, I.O.P., A.E.P., and R.O.; formal analysis, D.T. and C.T.; investigation, T.A., R.M.P., L.V., A.U, and C.T.; resources, I.O.P. and M.T.; writing—original draft preparation, I.O.P., A.E.P., R.M.P., and M.T. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
The study was approved by the Institutional Review Board (or Ethics Committee) of “Iuliu Hațieganu University of Medicine and Pharmacy”, Cluj-Napoca (no. 19/ 13.12.2016).
Footnotes
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.