How Frontal Lobe Brain Injury Can Affect an Individual
An Overview of Frontal Lobe Damage
Symptoms of dysfunction can be physical, behavioral, or cognitive
The frontal lobe is a large part of the brain. It extends from the front of the brain almost halfway to the back.
Damage to the frontal lobe can cause a range of symptoms. These can include behavioral problems, depression, and a loss of strength in the muscles.
A variety of conditions can damage the frontal lobe, including stroke, head trauma, and dementia.
This article discusses the frontal lobe of the brain, its functions, and the various conditions that can cause frontal lobe damage. It also discusses how frontal lobe damage is diagnosed and treated.
Where Is the Frontal Lobe and What Does It Do?
The brain has two hemispheres, or halves: left and the right. The hemispheres are divided into three sections: the forebrain, the midbrain, and the hindbrain.
Each section has specific functions:
- The hindbrain controls involuntary functions (ones that happen without your control) like respiration and heart rate.
- The midbrain is associated with coordination, alertness, vision, and hearing.
- The forebrain controls a range of social, emotional, and cognitive (thinking) functions, as well as motor function and memory.
SOURCES
- Sherwood CC, Smaers JB. What’s the fuss over human frontal lobe evolution? Trends Cogn Sci. 2013;17(9):432–433. doi:10.1016/j.tics.2013.06.008
- Cleveland Clinic. Brain: Temporal lobe, vagal nerve, & frontal lobe.
- Pirau L, Lui F. Frontal lobe syndrome. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2021.
- Olney NT, Spina S, Miller BL. Frontotemporal dementia. Neurol Clin. 2017;35(2):339-74. doi:10.1016/j.ncl.2017.01.008
- Sawyer RP, Rodriguez-Porcel F, Hagen M, Shatz R, Espay AJ. Diagnosing the frontal variant of Alzheimer’s disease: a clinician’s yellow brick road. J Clin Mov Disord. 2017;4(1):1-9. doi:10.1186/s40734-017-0052-4
- Korczyn AD, Vakhapova V, Grinberg LT. Vascular dementia. J Neurol Sci. 2012;322(1-2):2-10. doi:10.1016/j.jns.2012.03.027
- Li L, Liu J. The effect of pediatric traumatic brain injury on behavioral outcomes: a systematic review. Dev Med Child Neurol. 2013;55(1):37‐45. doi:10.1111/j.1469-8749.2012.04414.x
- Beynon R, Sterne JA, Wilcock G, et al. Is MRI better than CT for detecting a vascular component to dementia? a systematic review and meta-analysis. BMC Neurol. 2012;12:33. doi:10.1186/1471-2377-12-33
- Collins A, Koechlin E. Reasoning, learning, and creativity: frontal lobe function and human decision-making. PLoS Biol. 2012;10(3):e1001293. doi:10.1371/journal.pbio.1001293
- Model Systems Knowledge Translation Center (MSKTC). Emotional Problems After Traumatic Brain Injury.
Frontal Lobe Brain Injury
Introduction
The frontal lobe is a relatively large lobe of the brain, extending from the front of the brain almost halfway towards the back of the brain. Damage to the frontal lobe of the brain can cause a range of symptoms, including motor weakness and behavioural problems. A variety of conditions can damage the frontal lobe, including stroke, head trauma, and dementia[1].
Symptoms of damage to the frontal lobe can vary because of the many functions carried out by the frontal lobes. Symptoms may include one or more of the following:
- Weakness on one side of the body or one side of the face
- Falling
- Inability to solve problems or organize tasks
- Reduced creativity
- Impaired judgment
- Reduced sense of taste or smell
- Depression
- Changes in behaviour
- Low motivation
- Low attention span, easily distracted1
- Reduced or increased sexual interest or peculiar sexual habits
- Impulsive or risky behavior[1]
Anatomy
In evolutionary terms, the frontal cortex has been the most recent brain area to evolve. These lobes integrate the other brain areas and are particularly responsible for higher level thinking and cognitive skills such as planning, evaluating likely outcomes, multitasking, performing risk assessment and the niceties of social interaction; it is the area of the brain that deals with abstract concepts.
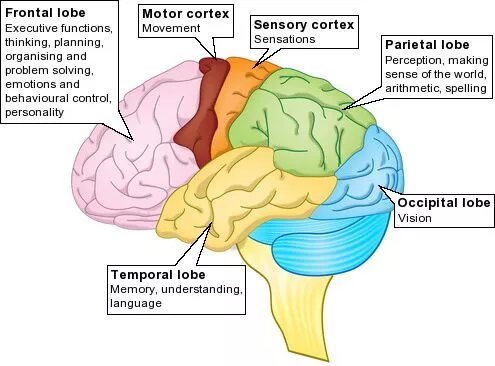
The frontal lobes account for approximately one-third of human brain mass. They lie at the front of the brain, anterior to the parietal lobes and superior to the temporal lobe. Each frontal lobe (left and right) is generally considered to have several distinct divisions:
- Motor cortex
- Premotor cortex
- Supplementary motor cortex
- Prefrontal cortex
- Orbital cortex AKA frontal eye fields
- Broca’s Area
Vascular supply
- Medial frontal lobe: anterior cerebral artery
- Deep & lateral regions: superior division of middle cerebral artery
Function

The frontal lobe modifies and imposes constraints on reflexive behaviours[2] and this control develops as the infant brain grows[3] and the frontal lobes become larger and more active.
- Motor cortex: voluntary movement
- Premotor cortex: storage of motor programs, sensorimotor integration, facilitation of controlled, smooth movements
- Prefrontal cortex: ability to concentrate; inhibition of reflexive behaviours; personality & emotional traits; abstract thinking. Working memory, executive functions including the ability to plan & implement (& monitor/evaluate) a series of goal-directed actions.
- Broca’s Area: Motor control of speech
- Supplementary Motor Cortex: Intentional preparation for movement, procedural memory
- Frontal Eye Fields: Control of voluntary scanning movements of the eye
Causes of Damage
- head injury (It has been found that in traumatic brain injury contusions typically occur on the poles and the inferior aspects of the frontal lobes[4].)
- stroke
- infection that affects the frontal lobe
- tumors in the frontal lobe
- multiple sclerosis
- neurodegenerative diseases eg Alzheimer’s disease, Parkinson’s disease, Huntington’s disease
Treatment and Rehabilitation
Treatment for damage to the frontal lobe depends on the cause. Frontal lobe damage treatment plans include a team of several types of healthcare professionals.
Some examples of potential treatments for frontal lobe damage include:
- Physical therapy to help maintain or regain mobility, strength, and flexibility.
- Occupational therapy to help learn new strategies to perform daily tasks and activities eg getting dressed, eating, or bathing.
- Vocational counseling.
- Speech-language therapy to aid in improving communication or teaching how to use assistive devices.
- Cognitive therapy, working on skills like planning, judgment, and memory.
- Psychological therapy to help improve relationships, emotional responses, and coping skills.
- Surgery may be recommended in cases when an injury or brain tumor is causing damage.
- In some cases, the cause of the frontal lobe damage may be permanent. eg neurodegenerative diseases. In these cases, treatment may also involve medications[5].
3 Frontal Lobe Syndromes
- Orbitofrontal syndrome – Lack of Inhibition. Patient demonstrates disinhibited, impulsive behaviour; difficulty in controlling their emotions; difficulty in maintaining concentration; lacking in judgement; failure to appreciate/anticipate consequences of their actions; can show euphoria, hypomania or grandiosity. Can also lead to abnormal sexual behaviour.
- Frontal convexity syndrome – Apathetic. Patient shows disinterest and is apathetic; slowing of motor functions; unable to plan ahead; lacks motivation; lacks concern about the world around them.
- Medial frontal syndrome – Akinetic. Reduced movement; loss of sensation in lower limbs; urinary incontinence; occasional mutism; profound apathy; sometimes show indifference to thirst or hunger
References
- ↑ Jump up to:1.01.1 Very well health Frontal lobe injuries Available from:https://www.verywellhealth.com/the-brains-frontal-lobe-3146196 (accessed 23.12.2020)
- ↑ Mesulam MM. The human frontal lobes: Transcending the default mode through contingent encoding. Principles of frontal lobe function. 2002 Jun 27;54:8-30.
- ↑ Luciana, ed. by Charles A. Nelson. Handbook of developmental cognitive neuroscience. Monica (2001). Cambridge, Mass. [u.a.]: MIT Press.
- ↑ Flint AC, Manley GT, Gean AD, Hemphill III JC, Rosenthal G. Post-operative expansion of hemorrhagic contusions after unilateral decompressive hemicraniectomy in severe traumatic brain injury. Journal of neurotrauma. 2008 May 1;25(5):503-12.
- ↑ Healthline Frontal lobe damage Available from:https://www.healthline.com/health/frontal-lobe#causes (accessed 23.12.2020)
Brain Trauma Can Cause Compulsive Sexual Desires
Frontal lobe damage and hypersexuality.
KEY POINTS
- Some may experience hypersexuality after brain trauma, as was the case with two women interviewed by ABC News.
- Hypersexuality causes dysfunction in the lives of people who have it and can be very distressing.
- Researchers continue to learn more about how a bump on the head can drastically change personality and cognitive abilities.
By Amy Broadway, researcher at the Brogaard Lab for Multisensory Research
Yesterday, ABC News posted this interesting story about how brain trauma spurred hypersexuality in two women. Brain trauma more often causes a decrease in libido. However, sometimes it causes an increase in libido, as in the case of Alissa, a 23-year-old who suffered a car accident, and Heather, a 43-year-old who suffered a subarachnoid hemorrhage.
An increase in sexual appetite may seem like fun, but as with other sexual disorders, hypersexuality causes dysfunction in the lives of people who have it and can be very distressing.

Alissa, who was a teenager at the time of her crash, had damage to her frontal lobe, the site in the cerebral cortex associated with executive functioning, including the capacity for self-control, foresight, attention, and reasoning. When the frontal lobe is damaged, so are a person’s executive functioning abilities, leading to psychological and emotional problems, such as perhaps hypersexuality. Perhaps because it is in the front of the head, it is a common site of injury for people who have been in car accidents.
Going from a typically functioning teenager who was not abnormally concerned with sex, Alissa started having constant, obsessive thoughts about sex. She felt as if she had no reason to live if she could not find a sex partner. She created an outlet for her urges by becoming a professional dominatrix and selling “sexy” videos of herself. She has not, however, enjoyed her sexual compulsions, but has merely tried to cope with them as best she can. Her urges have begun to subside with the help of medication and therapy.
Heather, married with children, became obsessed with sex while still hospitalized, asking her husband to have sex in the bathroom there. Afterward, she would blatantly proposition men, having sex with around 10 men and acting inappropriately with around 50. She was seemingly unaware that anything was improper about her behavior. Now she is also in therapy and on medication. Her husband, who was understanding enough to know her behavior was a result of the injury, has stuck by her through the ordeal.
Heather’s temporal lobe, hypothalamus, and amygdala were damaged by the hemorrhage. The hypothalamus and amygdala are located in the limbic system, which is deep in the temporal lobes. These structures are all associated with emotions. Injury to the amygdala and hypothalamus can result in disruption of normal hormonal functioning and the ability to inhibit behaviors. An inability to know what is appropriate behavior and a preoccupation with one’s sexual satisfaction may be connected with temporal lobe injury (Eghwrudjakpor, Essien, 2008).

Alissa and Heather’s stories highlight how important it is to protect our brains as best we can. Alissa put it well when she told 20/20:
I think that as people we’d like to think that our personality is a bit more stable than just, you know, like having, you know, a bump on the head be able to change that fundamentally.
Researchers are learning more and more how a bump on the head can drastically change personality and cognitive abilities.
References
Eghwrudjakpor, P., & Essien, A. (2008). Hypersexual Behavior Following Craniocerebral Trauma An Experience with Five Cases. The Libyan Journal of Medicine, 3(4), 192–194. doi:10.4176/080908
Symptoms Of Brain Injury
Any brain function can be disrupted by brain trauma: excessive sleepiness, inattention, difficulty concentrating, impaired memory, faulty judgment, depression, irritability, emotional outbursts, disturbed sleep, diminished libido, difficulty switching between two tasks, and slowed thinking.
Sorting out bonafide brain damage from the effects of migraine headaches, pain elsewhere in the body, medications, depression, preoccupation with financial loss, job status, loss of status in the community, loss of status in the family, and any ongoing litigation can be a formidable task.
The extent and the severity of cognitive neurologic dysfunction can be measured with the aid of neuropsychological testing. Neuropsychologists use their tests to localize and identify dysfunction to specific areas of the brain. For example, the frontal lobes play an essential role in drive, mood, personality, judgment, interpersonal behavior, attention, foresight and inhibition of inappropriate behavior. The ability to plan properly and execute those plans is known as “executive function.”
Frontal lobe injury is often associated with damage to the olfactory bulbs beneath the frontal lobes. Survivors may note a reduced, or altered sense of smell. One recent study (Varney 1993), showed that 92% of survivors of brain injury suffering anosmia (loss of smell) had ongoing problems with employment, even though their neuropsychological testing was relatively normal.
The effects of brain injury on the survivor may be equaled, or even surpassed, by the effect on the family. Brain injuries are known for causing extreme stress in family and interpersonal relationships. In general, the symptoms should lessen over time as the brain heals, but may worsen because of the survivor’s inability to accept help, or adapt to the brain injury. For this, and other reasons, it is not uncommon for psychological problems to surface, and worsen after brain injury.
SYMPTOM CHECKLIST:
Symptoms vary widely after “brain injury”, and the nature of them depends, in large part, on where the brain is injured. Below is a list of possible physical and cognitive symptoms which may arise from damage to specific areas of the brain:
FRONTAL LOBE: forehead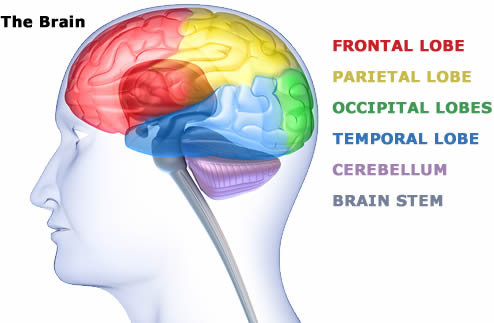
- Loss of simple movement of various body parts (Paralysis).
- Inability to plan a sequence of complex movements needed to
complete multi-stepped tasks, such as making coffee (Sequencing). - Loss of spontaneity in interacting with others.
- Loss of flexibility in thinking (Rigid Thinking).
- Persistence of a single thought (Perseveration).
- Inability to focus on task (Attending).
- Mood changes (Emotionally Labile).
- Changes in social behavior.
- Changes in personality.
- Difficulty with problem solving.
- Inability to express language (Broca’s Aphasia).
- Difficulty with serial tasking.
PARIETAL LOBE: near the back and top of the head
- Inability to attend to more than one object at a time.
- Inability to name an object (Anomia).
- Inability to locate the words for writing (Agraphia).
- Problems with reading (Alexia).
- Difficulty with drawing objects.
- Difficulty in distinguishing left from right.
- Difficulty with doing mathematics (Dyscalculia).
- Lack of awareness of certain body parts and/or
surrounding space (Apraxia) that leads to difficulties in self-care. - Inability to focus visual attention.
- Difficulties with eye and hand coordination.
OCCIPITAL LOBES: most posterior, at the back of the head
- Defects in vision (Visual Field Cuts).
- Difficulty with locating objects in environment.
- Difficulty with identifying colors (Color Agnosia).
- Production of hallucinations.
- Visual illusions – inaccurately seeing objects.
- Word blindness – inability to recognize words.
- Difficulty in recognizing drawn objects.
- Inability to recognize the movement of object (Movement Agnosia).
- Difficulties with reading and writing.
- Reduced peripheral vision.
TEMPORAL LOBES: side of head above ears
- Difficulty in recognizing faces (Prosopagnosia).
- Difficulty in understanding spoken words (Wernicke’s Aphasia).
- Disturbance with selective attention to what we see and hear.
- Difficulty with identification of, and verbalization about objects.
- Short term memory loss.
- Interference with long term memory.
- Increased and decreased interest in sexual behavior.
- Inability to catagorize objects (Categorization).
- Right lobe damage can cause persistent talking.
- Increased aggressive behavior.
- Ringing in the ear (Tinnitus).
BRAIN STEM: deep within the brain
- Decreased vital capacity in breathing, important for speech.
- Swallowing food and water (Dysphagia).
- Difficulty with organization/perception of the environment.
- Problems with balance and movement.
- Dizziness and nausea (Vertigo).
- Sleeping difficulties (Insomnia, sleep apnea).
CEREBELLUM: base of the skull
- Loss of ability to coordinate fine movements.
- Loss of ability to walk.
- Inability to reach out and grab objects.
- Tremors.
- Dizziness (Vertigo).
- Slurred Speech (Scanning Speech).