Covid-19 Vaccination Causing Stroke – Clots in Large Arteries Observed and Documented
First reported cases of clots in large arteries causing stroke following covid-19 vaccination 💉
Three cases of ischaemic stroke reported in young adults following administration of the Oxford–AstraZeneca vaccine
Clots in the arteries (arterial thrombosis) are the most common cause of stroke (ischaemic stroke) and have been reported in detail for the first time in young adults who received the Oxford–AstraZeneca covid-19 vaccine in a letter from UK stroke specialists published online in Journal of Neurology Neurosurgery & Psychiatry.
While rare cases of blood clots have been reported previously after administration of the Oxford–AstraZeneca covid-19 vaccine, these have affected veins and most specifically veins in the brain (cerebral venous sinuses).
People who have experienced this unusual form of stroke (cerebral venous sinus thrombosis) have also had low platelet counts (thrombocytopaenia) and antibodies to platelet factor 4 (PF4) – proteins that help form clots.
The most common form of stroke, where blood clots occur in arteries supplying blood to the brain (ischaemic stroke), has not been previously described as the presenting feature of thrombosis following administration of the Oxford–AstraZeneca vaccine, but the authors of this letter report three cases in detail.
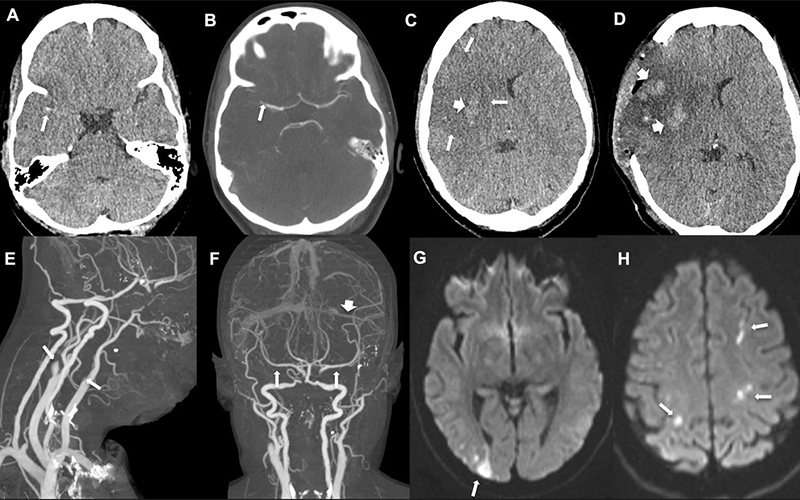
In all cases, the ischaemic stroke was associated with blockages of large arteries (both carotid and middle cerebral artery) and two patients also had venous thrombosis involving the portal and cerebral venous system. All three also had extremely low platelet counts, confirmed anti-PF4 antibodies, and raised D-dimer (also linked to clotting).
The first patient, a woman in her 30s, experienced an intermittent headache on the right side and around her eyes six days after the vaccine. Five days later she awoke feeling drowsy and with weakness to her left face, arm and leg. Imaging revealed a blocked right middle cerebral artery with brain infarction, and blood clots in the right portal vein thrombosis. She underwent brain surgery to reduce the pressure in her skull, plasma removal and replacement, and received the anti-clotting drug fondaparinux, but unfortunately died.
The second patient, a woman in her late 30s, presented with headache, confusion, weakness in her left arm and loss of vision on the left side 12 days after having received the vaccine. Imaging showed blockages in several vessels including both carotid arteries (the main blood supply to the hemispheres of the brain), arteries supplying the heart and lungs (pulmonary embolism) and the left transverse sinus (one of the cerebral venous sinuses). Her platelet count increased following plasma removal and replacement and intravenous corticosteroids. She was then given fondaparinux and improved.
The third patient, a man in his early 40s, presented 3 weeks after receiving his vaccination with problems speaking and understanding language (dysphasia). Imaging showed a clot in the left middle cerebral artery, but there was no evidence of clots in the cerebral venous sinuses. He received a platelet and plasma transfusion, and fondaparinux, and remains stable.
The lead author, Professor David Werring from the Stroke Research Centre, UCL Queen Square Institute of Neurology, says that the cases described suggest that, in addition to cerebral venous thrombosis, vaccine-induced immune thrombotic thrombocytopaenia (VTT) can also lead to clots that block arteries supplying the brain, causing ischaemic stroke.
“Young patients presenting with ischaemic stroke after receiving the [Oxford-AstraZeneca] vaccine should urgently be evaluated for VITT with laboratory tests (including platelet count, D-dimers, fibrinogen and anti-PF4 antibodies), and managed by a multidisciplinary team (haematology, neurology, stroke, neurosurgery, neuroradiology) for rapid access to treatments including intravenous immune globulin, methylprednisolone, plasmapheresis and non-heparin anticoagulants, for example fondaparinux, argatroban, or direct oral anticoagulants,” say the authors.
In a linked commentary, Professor Hugh Markus, from the Department of Clinical Neurosciences, at the University of Cambridge, writes: “This report emphasises that the immune mediated coagulopathy can also cause arterial thrombosis including ischaemic stroke, although venous thrombosis and especially cerebral venous sinus thrombosis appear more frequent.”
He adds: “During the current period of covid vaccination a high index of suspicion is required to identify thrombotic episodes following vaccination. However, it is important to remember that these side-effects are rare, and much less common than both cerebral venous thrombosis and ischaemic stroke associated with covid-19 infection itself.”
[Ends]
25/05/21
Notes for editors
Letter: Ischaemic stroke as a presenting feature of ChAdOx1 nCoV-19 vaccine-induced immune thrombotic thrombocytopenia doi: 10.1136/jnnp-2021-326984
Commentary: Ischaemic stroke can follow COVID-19 vaccination, but is much more common with COVID-19 infection itself doi: 10.1136/jnnp-2021-327057
Journal: Journal of Neurology Neurosurgery & Psychiatry
Funding: None declared
Link to AMS labelling system: https://press.psprings.co.uk/
Peer reviewed? Yes (internally)
Evidence type: Case studies; Opinion
Subjects: Stroke patients
source
💉Everyhting about – The COVID Vaccination💉 read here